Introduction
Depending on the type of undigested material, bezoars can be categorized as lactobezoars, pharmacobezoars, trichobezoars, and phytobezoars which include milk, medications, hair, and vegetables with high content of tannic acid, lignin cellulose, and hemicellulose, respectively [1,2]. In the case of phytobezoars, coagulation, and precipitation of tannic acid generates a gelatinous polymer that favors particle agglutination. Phytobezoar are a cause in 0.4%-4% of all mechanical bowel obstructions [1]. Bezoars are primarily diagnosed by imaging studies showing an oval mass with a clear boundary and a nonuniform internal density [3].
Invasive approaches such as surgical extraction through enterotomy or the placement of a decompression tube using endoscopy are available, but noninvasive approaches, including Coca Cola® injection to the bezoar, are more commonly used. In this report, we present the case of a giant bezoar successfully dissolved using an enzyme complex to illustrate the potential utility of a new alternative approach in cases where current interventions might fail [1,3-7].
Case presentation
A 67-year-old male patient presented with sweating and vomiting including traces of fiber. The patient was previously diagnosed with urothelial carcinoma and prostate adenocarcinoma six years ago, was treated with surgery and adjuvant radiotherapy, and developed radicular enteritis due to radiotherapy. Two years after cancer diagnosis, he was diagnosed with asymptomatic giant bezoar and was instructed to orally consume copious amounts of Coca Cola for several days, no programme of reviews was carried out to confirm resolution.
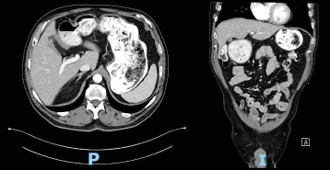
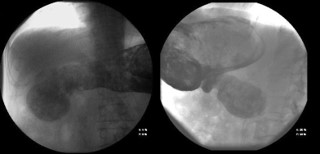
Computed Tomography (CT) scan performed at the time of admission revealed abundant food content with organized appearance in the abdomen (Figure 1), which was morphologically similar to that observed in previous CT scans. The findings supported chronic food retention with difficulty in gastric emptying at the level of pyloric antrum. Pharyngo-esophageal study revealed the presence of a bezoar occupying the entire gastric chamber with normal esophageal motility (Figure 2).
Based on the literature review [1,5,8-10], the patient was initiated treatment with the enzyme complex Digeston Plus® (HealthAid® House, Marlborough Hill, Harrow, Middlesex), which was administered once daily. According to the manufacturer, each pill (310 mg) was composed of the following enzymes and bacteria: 20,000 DU amylase, 50,000 HUT protease, 45 AGU glucoamylase, 50 endo-PGU pectinase, 225 GaIU alpha-galactosidase, 1000 ALU lactase, 30 BGU beta-glucanase, 1000 CU cellulase, 1000 FIP lipase CR, 125,000 FCCPU bromelain, 600 XU Xylanase, 400 HCU hemicellulase, 200 DP malt diastase, 203 SU invertase, 16,000 FCCPU papain, 120 mg calcium chloride, 20 mg mint extract, 10 mg papaya extract, 10 mg pineapple extract, 15 mg (300 million) Lactobacillus acidophilus, and 15 mg (300 million) Bifidobacterium longum.
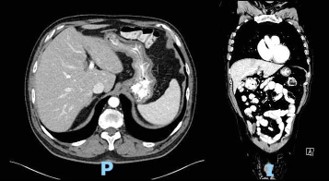
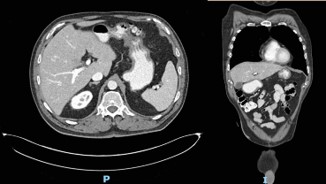
The patient followed an excellent clinical course, with full resolution of the symptoms after three months of treatment. The follow-up CT scan obtained three months (Figure 3) and six months (Figure 4) after admission revealed the complete dissolution of the bezoar. Annual clinical follow-up was performed until June 2025, with no recurrence of symptoms of bezoar reformation.
Discussion
Bezoars as factors in intestinal obstruction are a rare clinical presentation with variable incidence. Studies to date have identified several risk factors for bezoar development, including prior gastric surgery, Crohn disease, diabetes mellitus, dehydration, hypothyroidism, and renal failure, which can lead to reduced gastric motility and acidity. Bezoars can be asymptomatic or present as a variety of gastrointestinal symptoms, such as pain and abdominal fullness, depending on the location [2,3,7,10]. Gastric bezoars can trigger ulcerative lesions in the stomach and subsequent bleeding. Small intestinal bezoars accounts for approximately 0.4%-4% of all mechanical bowel obstructions.
Bezoar diagnosis is based on endoscopic or radiologic evaluation. Endoscopy plays the most important role in the detection as well as the treatment of gastric bezoars. CT is especially useful in patients requiring surgical removal of small intestinal bezoars [3,6,7]. The currently available treatment options for gastric phytobezoars include dissolution and removal with endoscopic devices or open surgery. Intestinal bezoars are generally treated using surgical procedures, since these patients often present with small bowel obstruction. Surgery is also reserved for cases where the density of the conglomerate renders noninvasive dissolution and endoscopic fragmentation is unfeasible. Recent studies have described gastrointestinal decompression with a nasogastric tube or a long intestinal tube in patients with acute small bowel obstruction without any signs of strangulation [3,4,6].
Dissolution is an efficient and less invasive approach in patients with large enteral feed bezoars. Cellulose, which is widely used for phytobezoar treatment, is not commercially available for ingestion or as a prescribed medication in many countries. Papain, which has been used as an alternative enzymatic therapy for bezoars, is associated with some adverse events such as gastric ulceration and esophageal perforation. In some patients, administration of prokinetic agents was reportedly effective in resolving gastric bezoars [5,7-11]. Several articles have highlighted the utility of Coca Cola® administration for the dissolution of phytobezoars [11]. A systematic review by Ladas et. al. revealed that Coca Cola® administration, alone or in combination with endoscopy, resulted in the resolution of phytobezoars in 91.3% of the cases and that this approach was more effective than cellulose and papain. Although the underlying mechanism has not been completely elucidated, Coca Cola® administration was not effective in the dissolution of the bezoar in the present case. Digeston Plus® is an enzyme complex that includes papain and cellulose in addition to pancreatic enzymes, which allows it to be a complete compound. As a commercially available product, its administration is feasible. Indeed, the present case illustrates the feasibility and efficacy of Digeston Plus® for the treatment of large gastric bezoars, providing a new treatment option for cases where which Coca Cola® is not effective and invasive treatment approaches are avoided, even when size and location are associated with suboclussive symptoms.
Declarations
Conflicts of interest and source of funding: The authors declare that they have no conflict of interest and no source of funding.
Ethical approval: All the procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The institutional ethics committee approved the publication of this case report.
Consent for publication: Oral informed consent was obtained from the patient for publication of this case report.
References
- Iwamuro M, Okada H, Matsueda K, Inaba T, Kusumoto C, Imagawa A, et al. Review of the diagnosis and management of gastrointestinal bezoars. World J Gastrointest Endosc. 2015; 7: 336.
- Sakellariou V, Andreadis I, Vaikousi E, Kolonis E. Phytobezoar: A rare cause of intestinal obstruction. Surg Chronicles. 2005; 10: 117–20.
- Park SE, Ahn JY, Jung HY, Na S, Park SJ, Lim H, et al. Clinical outcomes associated with treatment modalities for gastrointestinal bezoars. Gut Liver. 2014; 8: 400–7.
- Paschos KA, Chatzigeorgiadis A. Pathophysiological and clinical aspects of the diagnosis and treatment of bezoars. Ann Gastroenterol. 2019; 32: 224–32.
- Stanten A, Peters HE. Enzymatic dissolution of phytobezoars. Am J Surg. 1975; 130: 259–61.
- Li L, Xue B, Zhao Q, Xie HQ, Luan XR, Cui Q. Observation on the curative effect of long intestinal tube in the treatment of phytobezoar intestinal obstruction. Med (United States). 2019; 98.
- Vorovskiy OO, Shushkovska YY, Afanasiuk OI. Stomach bezoaris, causes of development, diagnosis and methods of treatment. Wiad Lek. 2021; 74: 128–31.
- Morell B, Buehler PK, Bader PR, Lang S, Scharl M, Gubler C, et al. Efficient treatment of esophageal nutrition bezoars: dissolution outmatches removal—the Zurich approach. Clin J Gastroenterol. 2021; 14: 1602–6.
- Gupta R, Fellow GI, Share M, Pineau BC. Dissolution of an esophageal bezoar with pancreatic enzyme extract. Gastrointest Endosc. 2001; 54: 96–9.
- Carreira Delgado M, Fernández Rodríguez E, Nuño VázquezGarza JM, Gil Llorens C, Vázquez López C. Oclusión intestinal por fitobezoar recidivante: resolución con tratamiento no operatorio mediante celulasa. Cir Esp. 2014; 92: 434–5.
- Ladas SD, Kamberoglou D, Karamanolis G, Vlachogiannakos J, Zouboulis-Vafiadis I. Systematic review: Coca-Cola can effectively dissolve gastric phytobezoars as a first-line treatment. Aliment Pharmacol Ther. 2013; 37: 169–73.