Introduction
The Omphalo Mesenteric Duct (OMD) serves as a conduit between yolk sac and gut of the developing fetus. During 8th week of gestation, the placenta develops and replaces the yolk sac as the source of fetal nutrition, with subsequent regression of OMD. However, in 1-4% of the population it fails to regress completely and result in wide spectrum of abnormalities which include: patent omphalo-mesenteric duct, omphalo-mesenteric cysts, Meckel’s diverticulum and congenital bands [1]. OMD cyst is further rare, may be intra or pre-peritoneal in location and generally results from obliteration of both the ends i.e umbilical and ileal ends, with cystic middle segment. It may be asymptomatic, get infected or cause bowel obstruction. Fifty percent of OMD related symptoms develop by 3 years of age, 75% by 10 years and presentation in adults and elderly is extremely rare [2,3]. Due to it’s rarity and varied presentation, pre-op diagnosis remains challenging especialy in elderly age group [4]. Radiological imaging like Ultrasound and CT abdomen aid in diagnosis but at times, it further adds to the confusion and creates a diagnostic dilemma. We hereby report a rare case of OMD cyst in an elderly male, presented as complicated para-umblical hernia, confirmed as omentocoele on Ultrasonography, but turned out to be a rare OMD cyst on surgical exploration.
Case report
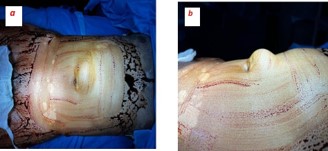
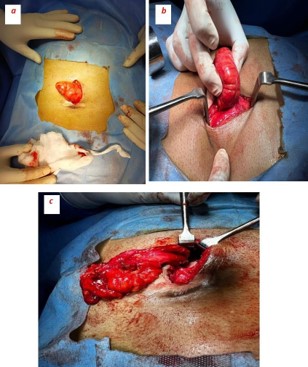
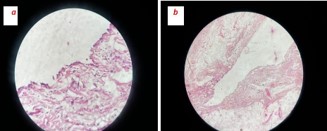
A 63-year-old male, farmer by occupation, presented with complaints of painful, irreducible, swelling in supra-umblical region since past four days. Both the symptoms observed simultaneously after lifting heavy weight. Pain was persistent, localized over the swelling and has mild to moderate in intensity. It was not associated with fever, vomiting, abdominal distension, constipation or obstipation. Patient did not have any history of previous abdominal surgery or ventral hernias. General physical examination was unremarkable. Abdominal examination revealed a 6 cm × 4 cm, well defined, firm, globular and tender swelling in mid-line just above the umbilicus (Figures 1a & 1b). There was no local rise of temperature and skin over the swelling was normal. Rest of the abdomen was scaphoid, nondistended, soft, nontender and bowel sounds were normal over all four quadrants of abdomen. Urgent laboratory investigation revealed leucocytosis (TLC12000/Cmm) with Neutrophil count of 80%. Other haematological and bio-chemical parameters were within normal limits. There was no dilated bowel loops, abnormal air-fluid levels or gas under diaphram on X-Ray chest and abdomen. Ultrasound abdomen, done at an outside centre, showed an extra-peritoneal cystic mass (Figure 2) without intraperitoneal extension, repeat ultrasound at our centre revealed a 13.6 mm size defect in anterior abdominal wall in supra-umbilical region with herniation of omentum and anechoic fluid collection in hernial sac suggestive of irreducible para-umblical hernia with omentocoele. In view of clinicoradiological suspicion of complicated ventral hernia, patient was taken up for emergency exploration under general anaesthesia via supraumblical mid-line incision. A ventral defect of approx 1.5 cm size was noticed in mid-line through which a cystic swelling of 6 cm × 5 cm was found protruding out which was attached to the ileum with a fibrous band (Figures 3a & 3b). The size of ventral defect was increased to deliver the content which was found attached to ileum with a fibrous band. The cyst along with its band was carefully dissected off the bowel, specimen (Figure 3c) was sent for histo-pathological examination, bowel was replaced back into the peritoneal cavity and ventral defect was repaired using nonabsorbable suture. Post op period was uneventful, patient was started on orals in the evening of surgery, discharged on 3rd post operative day and skin sutures were removed after ten days. Histopathological examination of specimen was reported as a unilocular cyst cavity lined by mesenteric type epithelium. The lining epithelium was surrounded by fibro-fatty tissue with psammoma bodies suggestive of OMD cyst (Figures 4a & b).
Discussion
Omphalo-mesenteric duct cysts are typically diagnosed in infancy or childhood, and their occurrence in elderly is exceedingly rare [3,5]. The age of our patient is 63 years, which is probably the eldest reported case of symptomatic OMD cyst in world literature. The OMD remnants has varied clinical presentation: it may present as acute abdominal conditions viz volvulus, intestinal obstruction, complicated hernia and meckel’s diverticulitis or chronic conditions like pain abdomen, rectal bleeding, umbilical fistula and umblical hernia. Our patient reported as complicated para-umblical hernia with painful and irreducible content. Ultrasonography and CT scan of the abdomen aid in diagnosis, but sometimes it adds to the confusion and final diagnosis is made only on surgical exploration. In our case, clinical and Ultrasound examination both were strongly suggestive of para-umblical hernia with omentocoel, hence CT abdomen was not asked for and patient was straight-way taken-up for surgical exploration and the diagnosis was confirmed only during laparotomy. Management of symptomatic OMD cyst is complete surgical excision, either laparoscopically or by open surgical approach, which serves both diagnostic and therapeutic purpose. The choice of surgical approach is usually dictated by the clinical condition of the patient, pre-op diagnosis and surgeon’s expertise [2,3]. In this reported case, the decision for an open surgical approach was guided by the clinical and radiological suspicion of complicated para-umbilical hernia, surgeon’s expertise as well as patient’s preference. The diagnosis was further substantiated by HPE report, which makes it a rarest of rare presentation of OMD cyst as a complicated para-umblical hernia in an elderly male.
Conclusion
Omphalo-mesenteric cyst presenting as acute abdomen in 6th decade of life is extremely rare. Preoperative diagnosis requires high index of suspicion as presentation may be deceptive. If remained undiagnosed, can lead to serious complications, hence timely diagnosis and appropriate management is of paramount importance.
Declarations
Conflict of interest: The authors declare that they have no conflict of interest.
Author’s approval: The manuscript has been read and approved by all the authors.
References
- Beasley SW. Vitellointestinal duct anomalies. In: Spitz L, Coran AG, editors. Operative Pediatric Surgery. 2013; 445–57.
- Sawada F, Yoshimura R. Adult case of an omphalomesenteric cyst resected by laparoscopic-assisted surgery. World J Gastroenterol. 2006; 12: 825–7.
- Annaberdyev S, Capizzani T. A rare case presentation of a symptomatic omphalomesenteric cyst in an adult, 25-year-old patient, treated with laparoscopic resection. J Gastrointest Surg. 2013; 17: 1503–6.
- Hu YY, Jensen T, Frinck C. Surgical condition of the small intestine in infants and children. In: Yeo CJ, editor. Shackelford’s Surgery of the Alimentary Tract. 8th ed. 2019; 970–90.
- Aktimur R, Yasar U. Extremely rare presentation of an omphalomesenteric cyst in a 61-year-old patient. Turk J Surg. 2017; 33: 43–4.