Case presentation
A 60-year-old male presented with several months of frequent throat clearing, persistent phlegm accumulation, and a sensation of saliva or mucus entering the airway, resulting in cough and choking. He described intermittent aspiration events occurring unpredictably, even while sitting upright. He reported frequent coughing fits, particularly when phlegm was present in the throat, as it would often “go down the wrong pipe” (larynx), triggering significant laryngeal cough reflex. His medical history was otherwise unremarkable, with no prior neurologic, esophageal, or pulmonary disease. A video fluoroscopic swallow study (modified barium swallow) was performed but did not indicate aspiration. However, the test used barium pudding (thick consistency), not thin liquids, which the patient reported as the true triggers for his aspiration episodes.
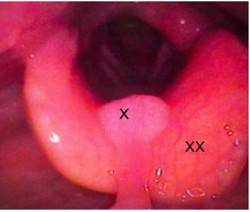
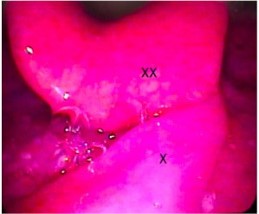
On fiberoptic laryngoscopy, string-like tissue was observed anterior to and partially encircling the epiglottis. The tissue was identified as a non-swollen, elongated uvula measuring nearly six inches, which obstructed the normal closure of the epiglottis during swallowing.
Discussion
Aspiration is most often caused by neurologic impairments such as stroke and Parkinson’s disease that disrupt swallowing [1]. In dementia, cognitive decline and impaired swallowing reflex increase the risk of aspiration by reducing airway protection [4]. Other well-described causes include structural or functional abnormalities such as Zenker’s diverticulum, strictures, esophageal dysmotility, oropharyngeal tumors, and impaired swallow coordination due to systemic disease [2]. Additionally, patients with chronic lung disease or gastroesophageal reflux disease may present with aspiration [3].
However, these commonly cited causes do not include an elongated uvula as a potential etiology [2]. In this patient, none of the common underlying conditions were present. There was no history of anaphylactic reaction. The absence of neurologic deficits, esophageal pathology, or head and neck masses made the findings on video laryngoscopy particularly notable. The nearly six-inch long uvula created a rare but significant mechanical obstruction to epiglottic closure, leading to aspiration events (Figures 1A & 1B).
This case highlights the importance of direct visualization via video laryngoscopy in patients complaining of aspiration or choking. Standard diagnostic tools, such a swallow study, may fail to reproduce symptoms, possibly due to the use of testing materials (solids vs. liquids). Recognition of this unusual anatomical cause is crucial, as it may be easily overlooked in favor of more common etiologies. Partial surgical removal of the uvula (uvulectomy) is expected to resolve the patient’s symptoms.
Conclusion
This case illustrates an unusual anatomical cause of chronic aspiration: An elongated uvula obstructing the epiglottis. Unlike the more common etiologies, this presentation was mechanical rather than neurologic or functional. Although a standard swallow study using barium pudding did not show aspiration, the patient continued to aspirate liquids and phlegm, leading to persistent coughing fits. The diagnosis was ultimately made through fiberoptic laryngoscopy, highlighting the value of direct visualization. The patient is scheduled to undergo a partial uvulectomy, which is anticipated to provide definitive symptom relief. Clinicians should remain alert to rare etiologies such as this, especially when patients exhibit aspiration symptoms not explained by conventional tests.
Declarations
Funding: Cedars Sinai Sinus Center.
References
- Almirall J, Boixeda R, de la Torre MC, Torres A. Aspiration pneumonia: a renewed perspective and practical approach. Respir Med. 2021; 185: 106485.
- Ficke B, Rajasurya V, Sanghavi DK, et al. Chronic aspiration. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2025.
- Sanivarapu RR, Vaqar S, Gibson J. Aspiration pneumonia. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2025.
- Yoshikawa H, Komiya K, Hamanaka R, Hiramatsu K, Kadota JI. Dementia as a risk factor for aspiration in patients with COVID-19. Geriatr Gerontol Int. 2021; 21: 757–8.