Introduction
The Foramen of Winslow (FoW) is a natural connection between the greater and lesser sacs of the peritoneum. It is bordered anteriorly by the hepatoduodenal ligament, posteriorly by the inferior vena cava, superiorly by the caudate lobe of the liver, and inferiorly by the duodenum. Despite being a relatively small communication, it is noted to be a rare and complicated site for herniation of the bowel.
Foramen of Winslow Hernias (FWH) account for only 8% of internal hernias and less than 1% of all hernias, according to the American College of Surgeons [1]. Due to its location and the small area involved, FWHs have been classically diagnosed intraoperatively or required urgent laparotomy/laparoscopy, occasionally requiring bowel resection. With only approximately 200 cases reported since it was first described, literature is often unclear about the standard of surgical care for affected patients.
Even less reported in literature are cases of spontaneous reduction of FWHs. In most reported cases, reduction was noticed during laparotomy, yet the decision to proceed with surgery was still made and resection of affected bowel was still performed.
We present a unique case of a spontaneously reducing foramen of Winslow hernia that subsequently did not require any surgical procedure. The patient was managed conservatively and ultimately discharged with follow-up.
Case presentation
Our patient is a 23-year-old female who presented to IUH Methodist Hospital in Indianapolis, Indiana. She came to the Emergency Department with complaints of acute onset right lower quadrant pain associated with nausea but no vomiting. She had no relevant past medical history, no prior surgeries, and no significant family history.
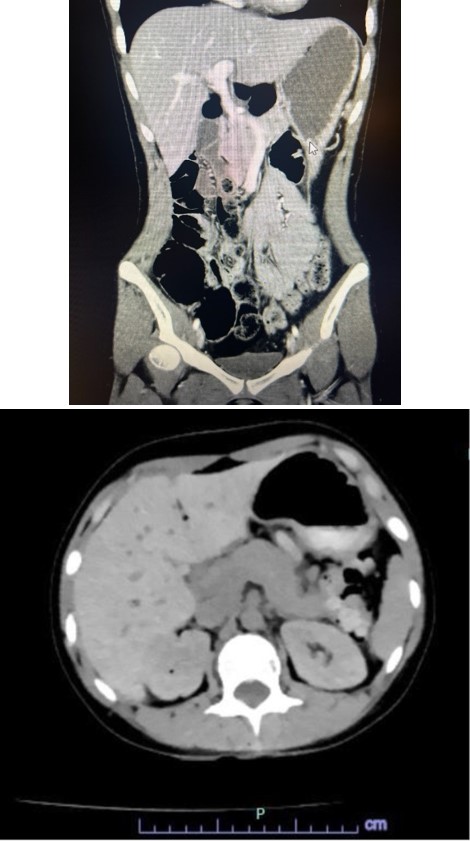
In the ED, labs and imaging studies were done to further assess her acute abdominal complaints. CBC was within normal limits and CMP revealed hyponatremia and hypokalemia. Urine pregnancy test and infectious disease workup were negative. CT abdomen with IV contrast revealed loops of small bowel and mesentery coursing between the celiac artery and portal vein with thinning and stretching of the main portal vein (Figure 1a). These findings suggested evidence of a foramen of Winslow hernia. General surgery was consulted and an operation was initially planned. However. upon repeat evaluation, the patient reported her pain and nausea had completely resolved. Review of systems, vitals, and physical exam at this time were completely negative. Repeat CT revealed oral contrast present throughout the small bowel without abnormal dilation (Figure 1b). These findings suggested spontaneous resolution of the suspected hernia. The plan at this time was to repeat labs and lactate, trial oral intake, and proceed with watchful waiting for recurrence/worsening of symptoms and clinical condition.
On the subsequent day, repeat labs were normal (including WBC and lactate). The patient passed her trial of oral intake without recurrence of symptoms. She was discharged with education on the etiology of her condition and instructed on strict return precautions.
Discussion
We looked closely at etiology and management of other reported cases of FWH. Current literature suggests that FWH etiology is associated with 3 main mechanisms(A) excessive viscera mobility, (B) abnormal enlargement of the foramen, and (C) changes in intra-abdominal pressure [2]. Enlargement of the right lobe of the liver and having undergone cholecystectomy have also been noted to be risk factors for FWH [2]. Loops of the small bowel are the most often to herniate, although cecal herniation and transverse colon herniation account for 30% and 7% of cases, respectively [2].
Review of literature also suggests that preoperative diagnosis of FWH is difficult. Physical exam, ultrasound, and abdominal radiographs can be useful tools but only diagnose around 10% of cases due to vague abdominal symptoms and nonspecific imaging findings [2]. Increased use of CT has led to better preoperative diagnoses. Still, in most cases, laparoscopy is used to visualize/diagnose the herniated bowel and allow for minimally invasive reduction [3,4]. The decision to perform more invasive surgery is made based upon the patient’s clinical presentation (i.e. evidence of bowel incarceration, bowel perforation, or inability to manually reduce hernia resulting in need for Kocher maneuver) [5]. FWH is frequently complicated by bowel ischemia and therefore can require converting to an open procedure and resecting the affected bowel [5].
Rarely, as seen with our patient, a FWH may spontaneously reduce. In almost all reported cases of this phenomenon, the decision to proceed with laparoscopy has still been made. In some cases, laparoscopic resection of a hypermobile segment of bowel was performed as prophylaxis for recurrence of herniation [6]. In other cases of spontaneous reduction, resection of the suspected affected bowel was done based on the bowel’s appearance and the patient’s clinical picture [7].
Conclusion
Current literature on surgical care and management of FWH is limited and often inconclusive. Recurrence of FWH has never been reported, yet many cases still are managed with prophylactic procedures, citing decreased risk of various sequelae. Even with spontaneously reducing hernias, most cases describe necessary procedures such as colopexy, hemicolectomy, or bowel resection for prophylaxis against potentially damaged and/or necrotic bowel. However, these procedures come with their own risks to patients, such as increasing length of stay, increased burden of medical cost, and potential damage to adjacent abdominal contents/subsequent need for additional procedures. Our case is unique in this aspect, showing conservative management of a patient with a spontaneously reducing hernia. Our patient was able to be discharged without undergoing additional procedures or accruing additional risk. Instead, her management can be guided by close follow-up. Existing literature makes us confident that recurrence is unlikely. Furthermore, her clinical picture reassures us that conservative management was the right choice. This case serves as an important development for considering conservative management for spontaneously reducing FWH.
References
- Overholt T, Crigger C, Robenstine J, Schaefer G. Ileocecal herniation into the lesser sac: a foramen of Winslow hernia. Am Coll Surg. 2019.
- Duinhouwer LE, Deerenberg E, Rociu E, Kortekaas RTJ. Herniation of the colon through the foramen of Winslow: a case report. Int J Surg Case Rep. 2016; 24: 14–7.
- Downs P, Downes N, Zayshlyy E, Esper C, Giuseppucci P. Internal hernia through the foramen of Winslow. J Surg Case Rep. 2018.
- Titan AL, Garagliano JM, Spain D. Management of an internal hernia through the foramen of Winslow. Trauma Surg Acute Care Open. 2022; 7: e000960.
- Moris D, et al. Foramen of Winslow hernia: a review of the literature highlighting the role of laparoscopy. J Gastrointest Surg. 2019; 23: 2093–9.
- Deschner BW, Schwulst SJ. Spontaneous reduction of acute cecal herniation through the foramen of Winslow. J Surg Case Rep. 2018.
- Cho HG, Kang J. Spontaneous reduction of small bowel herniation through the foramen of Winslow: importance of a timely approach. Ann Surg Treat Res. 2017; 92: 113–6.