Background
Meckel’s Diverticulum (MD), the most common congenital anomaly of the gastrointestinal tract, is associated with a mortality rate of approximately 10 % and high morbidity rates among survivors [1]. Most patients with MD remain asymptomatic, but children with the disease may develop symptoms of massive GI bleeding and rare complications, including intestinal obstruction, intussusception, hernia, inflammation, and perforation [2]. Small Bowel Obstruction (SBO) is a common surgical condition, accounting for 50 % of emergency laparotomies annually in the UK and over 300,000 admissions annually in the United States of America (USA) [1].
Schistosoma mansoni infection causes diffuse inflammation of the intestinal wall and destruction of the enteric nervous system. Clinically, the patients usually present with anemia, bloody diarrhea, and vague abdominal pain [3,4]. Rarely present as intestinal obstruction.
Herein, we present a case of 29 years adult male who has schistosomiasis mansoni in Meckle’s diverticulum, resulting in intestinal obstruction.
Case presentation
A 29-year young, healthy male presented with sudden onset abdominal pain lasting for 8 hours, generalized, colicky in nature, associated with one-time vomiting and anorexia. On examination, vital signs were normal apart from tachycardia of 104 b/min; the abdomen was distended, with generalized tenderness, tympanic on percussion, positive bowel sound, and digital rectal examination showed an empty rectum.
The patient was resuscitated and kept nothing by mouth (NPO). Complete Blood Count (CBC) showed leukocytosis of 16.33, while others were normal; abdominal x-ray shows dilated small bowel loops and multiple air-fluid levels.
CT reported a markedly distended stomach and small bowel with no clear area of transition zone that could be seen; multiple enlarged mesenteric lymph nodes and engorgement of mesenteric vessels are noted, mainly at the mid and left abdomen (Figure 1).
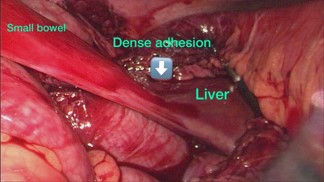
As there is a high suspicion of bowel obstruction on a virgin abdomen, underwent diagnostic laparoscopy, the intraoperative there is significant dilatation of the small bowel with minimal serous fluid seen in the pelvis. The inflammatory band was present at the distal part of the diverticulum and found twisting the bowel around itself and attaching to the liver edge segment (IV-B) (Figure 2).
The band was released, and wedge resection of the diverticulum was performed at its base by Gastrointestinal Anastomosis (GIA) on healthy tissue, about 2 cm from the inflamed segment, a standard surgical approach for MD. The postoperative period was uneventful. The patient was kept on a regular surgical floor and discharged on the second postoperative day after passinga bowel motion.
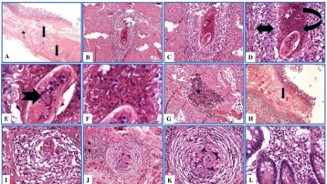
The specimen consisted of a 22 cm long segment of the small intestine (circumference 3 cm) with dull serosa and granular mucosal surface. No mucosal masses, polyps, or ulcers were seen. On histology, there was an increased density of mixed inflammatory cell infiltrate in the lamina propria. Multiple eosinophilic microabscesses (dense aggregates of eosinophils) and granulomata were seen in the submucosa and the muscularis propria. They included cellular (abundant epithelioid histiocytes with scant fibroblasts), fibro cellular (admixture of both epithelioid histiocytes with scant fibroblasts), and fibrotic (scant epithelioid histiocytes with abundant fibroblasts) granulomas. An intensely eosinophilic material (Splendore-Hoeppli phenomenon) and mixed inflammatory cells were seen surrounding the ova. A summary of these findings is shown in Figure 3.
The patient has referred afterward to the infectious disease department for initiation of praziquantel, which is the drug of choice for schistosomiasis and is effective against all Schistosoma species.
Discussion
Meckel’s diverticulum is the most common congenital malformation of the GI tract caused by incomplete obliteration of the vitelline (omphalomesenteric) duct. Prevalence in 2% of the population; 2% are symptomatic, children are usually less than two years, affects males twice as often as females, is located 2 feet proximal to the ileocecal valve, is 2 inches long or less, and can have two types of the mucosal lining [5,6]. Complications of Meckel’s diverticulum have been reported to occur in 4-40% of patients. They can include GI bleeding, intussusception, intestinal obstruction, diverticulitis, enteroliths, perforation, rarely vesica-diverticular fistula, and tumors [7]. Among these complications, GI bleeding occurs predominantly in children, while inflammation and obstructions tend to occur in adults [8,9].
Schistosomiasis is a leading global health issue affecting more than 200 million people worldwide, particularly with the epidemic spreading in tropical areas [10]. Schistosomiasis Mansoni is a major health problem in the Middle East, South America, the Caribbean, and sub-Saharan Africa [11]. Our case was found to have S. mansoni in histopathology.
The lifecycle of schistosomiasis starts with eggs in the urine or feces released to the freshwater environment from an infected host. After hatch, miracidia typically infect the intermediate host snail, in which infectious cercariae are maturated, amplified, and released into freshwater [10].
Adult S. mansoni worms in the liver’s blood vessels migrate from the hepatic portal vein into the superior mesenteric vein. From the superior mesenteric vein, the parasites could otherwise move via the jejunal and ileal veins to the venules draining the small intestine (jejunum and ilium) to lay eggs. Moreover, The Schistosoma mansoni adult pairs migrate to the venous vasculature surrounding the intestines; eggs laid here can pass through the blood vessel wall, intestine wall, and intestinal lumen. The parasite eggs are deposited throughout the entire intestinal tract of infected experimental animals [3,4,12]. Immunopathological reactions against schistosome eggs trapped in host tissues lead to inflammatory and intestinal obstruction, hepatosplenic inflammation, and liver fibrosis [13].
Diagnosis of schistosomiasis Mansoni is based on microscopic examination of the stools or biopsies from the intestinal lesions. Clinically, the patients usually present with anemia, bloody diarrhea, and vague abdominal pain [3,4]. Many infected people suffer from motility-related gastrointestinal problems; the diffuse mucosal inflammation causes an increase in the thickness of the mucosa, with blunting of the villi [14].
Almadi et al. reported a case of intestinal obstruction secondary to MD complicated by Schistosoma mansoni in middle age Egyptian males [11]. Similarly, our case had an infrequent presentation as an acute intestinal obstruction in the virgin abdomen; he was treated with laparoscopic exploration and praziquantel after surgery; histopathology shows Schistosoma in the Meckles diverticulum.
Conclusion
Diagnostic laparoscopy should be considered for all patients having a virgin abdomen presenting with complete bowel obstruction. To the best of our knowledge from the literature review, this is the second reported case of acute intestinal secondary to MD harboring Schistosoma mansoni.
References
- Lee MJ, Sayers AE, Drake TM, et al. National prospective cohort study of the burden of acute small bowel obstruction. BJS Open. 2019; 3: 354–366.
- Tuasha N, Hailemeskel E, Erko B, Petros B. Comorbidity of intestinal helminthiases among malaria outpatients of Wondo Genet health centers, southern Ethiopia: implications for integrated control. BMC Infect Dis. 2019; 19: 659.
- Hussein MR, Abu-Dief EE, El-Hady HA, Mahmoud SS, Salah EM. Quantitative comparison of infected Schistosomiasis mansoni and Haematobium: animal model analysis of the granuloma cell population. J Egypt Soc Parasitol. 2005; 35: 467–476.
- Hussein MR, Nassar MI, Kamel NA, Osman ME, Georguis MN. Analysis of fibronectin expression in the bilharzial granulomas and of laminin in the transformed urothelium in schistosoma haematobium infested patients. Cancer Biol Ther. 2005; 4: 676–678.
- Hansen CC, Søreide K. Systematic review of epidemiology, presentation, and management of Meckel’s diverticulum in the 21st century. Medicine. 2018; 97: e12154.
- Francis A, Kantarovich D, Khoshnam N, Alazraki AL, Patel B, Shehata BM. Pediatric Meckel’s Diverticulum: report of 208 cases and review of the literature. Fetal Pediatr Pathol. 2016; 35: 199– 206.
- Kusumoto H, Yoshida M, Takahashi I, Anai H, Maehara Y, Sugimachi K. Complications and diagnosis of Meckel’s diverticulum in 776 patients. Am J Surg. 1992; 164: 382–383.
- Yahchouchy EK, Marano AF, Etienne JCF, Fingerhut AL. Meckel’s diverticulum. J Am Coll Surg. 2001; 192: 658–662.
- Mackey WC, Dineen P. A fifty-year experience with Meckel’s diverticulum. Surg Gynecol Obstet. 1983; 156: 56–64.
- Shuja A, Guan J, Harris C, Alkhasawneh A, Malespin M, De Melo S. Intestinal schistosomiasis: a rare cause of abdominal pain and weight loss. Cureus. 2018; 10: e2086.
- Almadi F, Aljohani E. Rare cause of complicated Meckel’s with Schistosoma infection: an unusual cause of acute intestinal obstruction in adults. Int J Surg Case Rep. 2020; 66: 257–259.
- Nation CS, Da’dara AA, Marchant JK, Skelly PJ. Schistosome migration in the definitive host. PLoS Negl Trop Dis. 2020; 14: e0007951.
- McManus DP, Bergquist R, Cai P, Ranasinghe S, Tebeje BM, You H. Schistosomiasis – from immunopathology to vaccines. Semin Immunopathol. 2020; 42: 355–371.
- Bogers J, Moreels T, De Man J, et al. Schistosoma mansoni infection causing diffuse enteric inflammation and damage of the enteric nervous system in the mouse small intestine. Neurogastroenterol Motil. 2000; 12: 431–440.