Background
Urothelial Carcinoma (UC) recurrence via pagetoid spread to the vulva is rare and poorly characterized. The pagetoid spread refers to intraepithelial dissemination of tumor cells mimicking extramammary Paget's disease, complicating the diagnosis and clinical management. These cases have been reported infrequently, posing significant diagnostic and management challenges due to its unusual localization and overlap with other vulvar malignancies [1].
Histologically, pagetoid spread of UC can be diagnosed via skin biopsy. Microscopically, it involves tumor cells that are large, with abundant pale cytoplasm, and infiltrate the basal and parabasal layers of the squamous epithelium. These tumor cells express markers consistent with urothelial origin, such as GATA3, CK7, and uroplakin, while also being negative for melanoma and squamous markers, assisting in differentiation from other vulvar neoplasms.
Treatment for pagetoid recurrence remains poorly established. Surgical resection can be challenging, especially in the setting of recurrence, as many patients may have already undergone multiple radical resections or radiation treatment. The roles of chemotherapy and radiation are often limited in these scenarios favoring secondary radical procedures [2].
The following report presents a unique case of UC with pagetoid spread to the vulva and anus in a postmenopausal wom-an-a rare manifestation of this disease requiring an infralevator exenteration following previous radical resections and pelvic irradiation.
Case presentation
A 70-year-old woman with a history of recurrent UC presented to gynecology oncology office for increased pruritus, tenderness and new onset vaginal spotting for 3 months. She denied trauma, vaginal dilator uses or sexual activity. She underwent a trial of topical estrogen, Silvadene cream, Aquaphor cream, and Neosporin at various times to the vulvar area without relief.
In 2014, the patient was diagnosed with high grade TisNOMO urothelial carcinoma of bladder at the time of right ureteral stone extraction. In 2015, she underwent radical cystectomy, total abdominal hysterectomy, bilateral salpingo-oophorectomy, creation of Hautmann ileal neobladder, bilateral pelvic lymph node dissection, omental pedicle flap after treatment failure of intravesical BCG therapy. Final pathology demonstrated a microscopic positive margin at the urethra which was observed.
Following radical cystectomy, in the setting of recurrent Clostridium difficile infections, she developed an entero-neobladder fistula. This was complicated by serial neobladder stones requiring laser lithoplaxy. In 2021, she underwent an exploratory laparotomy, excision of fistula tract, left ureteral reimplantation and cystogram.
However, within 6 months, CT imaging demonstrated a new nodular enhancement at the junction of the urethra and neobladder concerning for recurrent disease. Genitourinary tumor board consensus was for neoadjuvant chemotherapy with pelvic radiation followed by anterior exenteration that included urethrectomy, excision of anterior vagina with neo-bladder and creation of ileal conduit. Final pathology demonstrated poorly differentiated carcinoma involving invasion at the neck of the neobladder with negative ureteral, urethral and peripheral soft tissue margins.
Clinical course
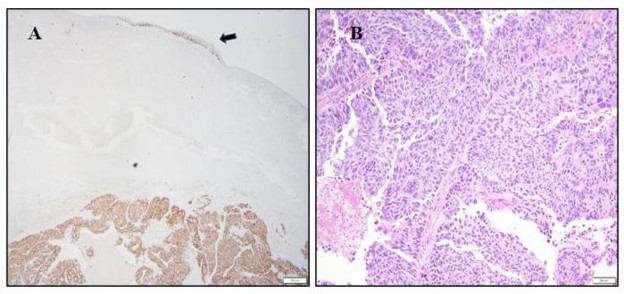
In July 2024, in the absence of visible vulvo-vaginal pathology and ongoing symptoms, patient underwent targeted gynecologic biopsies which confirmed pagetoid recurrence of urothelial carcinoma of the right lower vulva. PET-CT and MRI confirmed no extrapelvic evidence of metastases. She was then taken to the operating room for mapping biopsies to assess extent and distribution of cutaneous recurrence along the vulva, perineum and anus (Figure 1a). On interval examination, clitoromegaly was now obvious with a blooming vulvar erythema expanding to perineum and circumferentially on the anus, which presented positive for Pagetoid spread on final section (Figure 1b). In October 2024, following Gynecologic Oncology tumor board consensus, she underwent posterior pelvic exenteration including total radical vulvectomy, clitorectomy, completion vaginectomy, end colostomy, and myocutaneous flap reconstruction. Final pathology demonstrated invasive carcinoma into the clitoris and right vulva with pagetoid spread of the carcinoma affecting the left and right vulvar skin, introitus, and perianal skin extending into anal canal up to the pectinate line. Peripheral skin, vaginal and colonic margins were all negative.
Histopathological and Immunohistochemical Findings
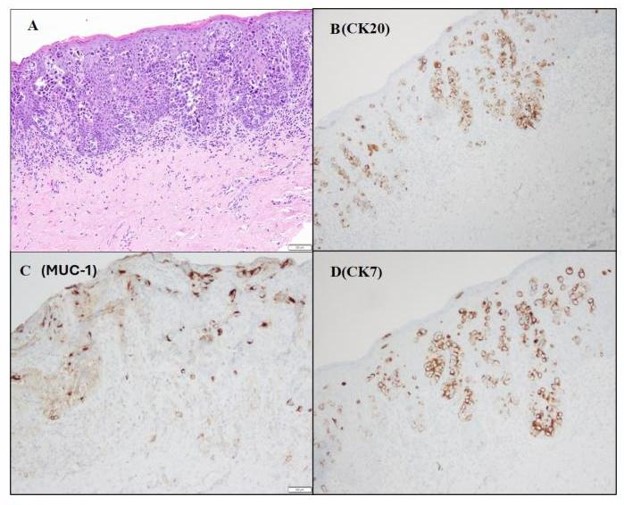
The primary biopsy displayed morphological characteristics indicative of urothelial carcinoma with pagetoid changes in the underlying squamous mucosa with cells positive for CK20, MUC-1 (Figure 2), GATA-3. Focal lymphovascular space invasion was identified. Immunohistochemical stains noted positivity for GATA-3, CK7, CK20, MUC1, and p63, while negative for uroplakin and CK5/6. This staining profile is well-documented in cases of secondary Paget's disease. Despite uroplakin negativity, tumor cells showed reactivity for MUC1, consistent with the stage and aggressiveness of the tumor, as described in the literature. The right periclitoral area displayed 1.5 cm area of invasion with a margin of 1.5 cm from the right and posterior skin. The pagetoid region displayed negative skin margins .
Discussion and conclusions
Diagnosis
Vulvar Paget Disease (VPD) is an uncommon cutaneous adenocarcinoma of the vulva, representing 1-2% of vulvar neoplasms and primarily affecting postmenopausal women. The vulva is the most prevalent site of occurrence (60-80%), followed by the perineal area (15%) and male genitalia (14%). The condition presents with nonspecific symptoms like itching and eczematous lesions, often resembling chronic eczematous disorders, which can lead to misdiagnosis as a benign skin issue [3]. Accurately distinguishing between primary and secondary diseases is vital for effective treatment. Primary vulvar Paget's disease originates from the epidermis and can be categorized as in situ or intraepithelial (usual type), invasive, or associated with an underlying adenocarcinoma of a skin appendage. In rare instances, primary Paget's disease may arise from dermal apocrine glands and extend into the overlying epidermis [4]. Conversely, secondary vulvar Paget disease emerges from metastatic spread to the epidermis, typically originating from anorectal, urothelial, or other adenocarcinomas [5]. Pagetoid spread of Urothelial Carcinoma (UC) is regarded as a rare condition with only approximately 15 prior cases reported in the literature, 5 of which were females [1,2,6-9]. Given this, documentation of UC with pagetoid spread treatment is limited due to its infrequency [5]. This type of spread usually involves the
migration of neoplastic cells along the adjacent epithelium, which can extend into squamous or glandular metaplasia of the urothelium. Proper biopsies from representative lesions with comparison to primary diagnostic biopsies are crucial for accurate diagnosis and differentiation from primary vulvar neoplasms or other malignancies [3].
Histopathological features of primary Paget disease include atypical cells with large nuclei, prominent nucleoli, and infrequent mitosis distributed throughout the epithelium, while the pagetoid spread of UC presents with disorganized or pleomorphic cells with mitotic activity that resembles high-grade urothelial cells with hyperchromatic nuclei [1,8]. To distinguish primary Paget's disease from UC with pagetoid spread in the lower genital tract, a specific immunoprofile is essential due to the similar morphologic patterns of both conditions. Immunohistochemistry plays a key role in differentiating primary Paget's disease, which typically exhibits CK7, allowing it to be distinguished from cells associated with high-grade squamous intraepithelial lesions, HPV-independent VIN, and vulvar melanoma; however, this distinction does not apply to urothelial cells, which are also CK7 positive. Markers such as EMA, CAM5.2, CEA, and GATA3 are generally diffusely positive in UC, while uroplakin-3, CDX2, and CK20 are generally negative (though occasional cases may show focal positivity for CK20) [8]. The expression of these markers may indicate a secondary origin of vulvar skin due to urothelial carcinoma or rectal adenocarcinoma [3,10]. Paget's disease secondary to anorectal carcinoma shows immunoreactivity for CK20 but is usually nonreactive for CK7 and does not express GCDFP-15 [10]. In contrast, vulvar Paget's disease secondary to UC is positive for CK7 and CK20 but negative for GCDFP-15. Conversely, markers such as uroplakin II/III, GATA3, and the coexpression of CK7 and CK20 are indicative of pagetoid spread of urothelial intraepithelial neoplasia, confirming the urothelial origin [11]. Uroplakin has been noted to be useful in differentiating between these two origins because it is specific to urothelium [11]. However, its sensitivity varies from 22% to 75% in cases of invasive and metastatic cancer, and the absence of uroplakin expression in invasive UC is significantly associated with advanced pathologic stage [11]. Invasive urothelial adenocarcinoma has shown immunoreactivity for MUC1, with elevated levels correlating with tumor invasion and metastasis across various carcinomas [12].
Treatment
The optimal treatment for pagetoid recurrence remains undefined due to the rarity of reported cases and incomplete treatment data. Of the cases reviewed in the literature, there is insufficient consensus to determine the efficacy of chemotherapy compared to surgery and/or the role of radiation. In our case, the patient had previously undergone several surgical excisions followed by chemoradiation therapy in conjunction with radical surgical excision. Her prior history of definitive radiation and perianal involvement excluded the option of further radiation. Surgical excision over chemotherapy was favored by her primary genitourinary oncologist given the multiply recurrent pattern of this disease. Considering her extensive surgical history, a radical surgical approach was necessary resulting in a diagnosis of definitive invasion surrounded by pagetoid spread along the clitoris, labia minorum, part of the labia majorum, perineum, and anus. Despite these challenges, the patient tolerated the procedure well and negative surgical margins were achieved. She continues without evidence of disease. This case provides valuable insights into the management of this rare urological recurrence, contributing to the limited body of evidence available.
Conclusion
Vulvar Paget's disease, particularly when associated with pagetoid spread from UC presents a significant diagnostic and therapeutic challenge. Secondary vulvar Paget's disease resulting from UC occurs when neoplastic cells migrate along the epithelium, potentially extending into areas of squamous or glandular metaplasia. It is crucial to differentiate secondary vulvar Paget's disease from the primary form to optimize treatment. Radical re-excision may be considered but it remains unclear if negative margin status leads to longstanding disease-free interval.
This case underscores the importance of integrating clinical, histological, and immunohistochemical data to achieve an accurate diagnosis. The presence of pagetoid spread may mimic other vulvar pathologies, such as extramammary Paget's disease or melanoma, necessitating the use of specific urothelial markers for differentiation.
Given the identification of bladder urothelial carcinoma as the primary tumor, management involved systemic therapy and radical surgical excisions for urothelial carcinoma and close monitoring of the vulvar lesion. Multidisciplinary care, including urologic oncology, gynecologic oncology, and dermatopathology, is essential for optimizing outcomes in such complex cases.
This case highlights the diverse presentations of urothelial carcinoma and the need for awareness of rare manifestations like pagetoid spread to the vulva, expanding the spectrum of urothelial carcinoma pathology.
Declarations
Ethics approval and consent to participate: Ethical approval was waived due to the nature of this case report.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Availability of data and materials: All relevant clinical data and histological findings are included within the manuscript. Additional clinical and histological data may be available upon reasonable request.
Competing interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding: No funding was received for this case report.
Authors' contribution: Maya Yasukawa: Writing - review & editing, Writing - original draft, Data curation. Lidys Rivera: Writing - review & editing, Michael A. Poch: Writing - review & editing, Robert M Wenham: Writing- review & editing, Ardeshir Hakam: Writing - review & editing. Monica Avila: Writing - review & editing, Writing - original draft, Supervision, Project administration, Methodology, Data curation, Conceptualization.
References
- Lu, B. and Y. Liang, Pagetoid spread of bladder urothelial carcinoma to the vagina and vulva. J Low Genit Tract Dis. 2015; 19: e13-6.
- Yamamoto S, et al. Pagetoid spread of urothelial carcinoma controlled without resection. UU Case Rep. 2023; 6: 65-69.
- van der Linden M, et al. Paget disease of the vulva. Crit Rev Oncol Hematol. 2016; 101: 60-74.
- Wilkinson EJ, HM Brown. Vulvar Paget disease of urothelial origin: a report of three cases and a proposed classification of vulvar Paget disease. Hum Pathol. 2002; 33: 549-54.
- Caruso G, et al. Vulvar Paget's Disease: A Systematic Review of the MITO Rare Cancer Group. Cancers (Basel). 2023: 15.
- Lopez-Beltran A, et al. The pagetoid variant of bladder urothelial carcinoma in situ A clinicopathological study of 11 cases. Virchows Arch. 2002; 441: 148-53.
- Tokuoka K, et al. A case of pagetoid spread of urothelial carcinoma with notable reduction achieved through enfortumab vedotin, resulting in complete surgical resection. Int Cancer Conf J. 2024; 13: 510-514.
- Koyanagi Y, et al., Detection of pagetoid urothelial intraepithelial neoplasia extending to the vagina by cervical screening cytology: a case report with renewed immunochemical summary. Diagn Pathol. 2019; 14: 9.
- Padhy RR, N Nasseri-Nik, F Abbas. Poorly differentiated highgrade urothelial carcinoma presenting as Paget's disease of the vulva with no overt urinary tract neoplasm detected. Gynecol Oncol Rep. 2017; 20: 70-72.
- Kristoffersen HL, R Roge, S Nielsen. Comparison of Antibodies to Detect Uroplakin in Urothelial Carcinomas. Appl Immunohistochem Mol Morphol. 2022; 30: 326-332.
- Brown HM, EJ Wilkinson. Uroplakin-III to distinguish primary vulvar Paget disease from Paget disease secondary to urothelial carcinoma. Hum Pathol. 2002; 33: 545-8.
- Stojnev S, et al. Prognostic significance of mucin expression in urothelial bladder cancer. Int J Clin Exp Pathol. 2014; 7: 4945-58.