Background
Headache is one of the most frequently reported medical complaints. According to the International Classification of
Headache Disorders (ICHD-3, 2018), headaches are categorized into primary, secondary, cranial neuropathies, and other facial
pains [1]. Over 90% of primary headaches fall into common subtypes such as migraine, tension-type headache, and cluster
headache [2].
When a headache is caused by an identifiable underlying condition, it is classified as a secondary headache. Some of the most frequent
causes of secondary headaches include thunderclap headaches (associated with subarachnoid hemorrhage, reversible vasoconstriction syndrome,
venous sinus thrombosis, and cervical artery dissection), idiopathic intracranial hypertension, intracranial hypotension, medication-induced
headaches, temporal arteritis, intracranial tumors, and central nervous system infections [3].
Vertebral artery dissection is a critical differential diagnosis in any patient presenting with a new-onset headache, with or without
neurological symptoms, especially in the context of recent neck manipulation or trauma. The clinical outcomes of vertebral artery dissection
can vary significantly, ranging from full recovery with no lasting deficits to severe complications or even death. This case report discusses
a rare presentation of bilateral vertebral artery dissection following chiropractic neck manipulation, highlighting the importance of early
recognition and intervention to prevent serious outcomes.
Case Report
A 30-year-old Caucasian woman with no significant past medical history presented to the Emergency Department (ED) with persistent occipital headache and nausea that developed immediately after chiropractic neck manipulation. Two weeks prior, she had sustained a minor neck injury, which led to ongoing neck pain. Seeking relief, she visited a chiropractor, where she underwent cervical spinal manipulation. Shortly after the procedure, she developed a new-onset headache, which persisted despite symptomatic treatment. She was initially evaluated by her primary care physician and prescribed pain medications and muscle relaxants, but the symptoms continued. Four days after the manipulation, she presented to the ED due to persistent headaches and neck pain. Her home medications included Norco 5 mg every six hours as needed for pain and Flexeril 5 mg every eight hours as needed for muscle spasms. She denied alcohol, tobacco, or illicit drug use and had no personal or family history of connective tissue disorders, stroke, or vascular disease.
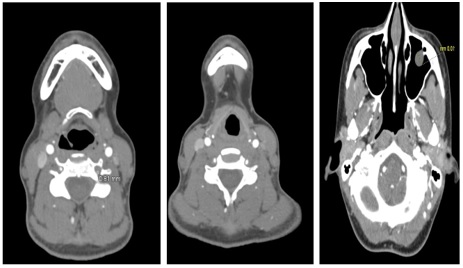
On examination, vital signs were stable, extraocular movements and visual fields were intact, and cranial nerves II-XII were normal. Neck flexion was limited due to pain, but no focal neurological deficits were noted. Given her headache following cervical manipulation, the differential diagnosis included tension headache, migraine, occipital neuralgia, and cervical artery dissection. Laboratory tests, including Complete blood count, Complete metabolic panel, C-reactive protein, erythrocyte sedimentation rate, and ANA screen, were unremarkable (Table 1). CT angiography (CTA) of the head and neck with contrast revealed bilateral vertebral artery stenosis suggestive of vertebral artery dissection (Figure 1). She was started on a heparin drip for anticoagulation, and neurology and interventional neurology were consulted, who recommended conservative management. She was discharged on day three with warfarin therapy and reported improvement in her headache. Follow-up imaging at six months showed healing of the dissections, and she remained neurologically intact. Warfarin was discontinued at her six-month follow-up, and she was transitioned to long-term antiplatelet therapy with aspirin.
Table 1: Complete blood count, complete metabolic panel and other chemistries.
| Description |
Result |
Normal Range |
Units |
| Complete blood count |
| WBC count |
8.93 |
4.10-12.20 |
10^3/uL |
| RBC count |
4.66 |
4.40-5.50 |
10^6/uL |
| Hemoglobin |
12.4 |
12.2-16.7 |
g/dL |
| Hematocrit |
37 |
38.2-49.2 |
% |
| MCV |
81.9 |
77.8-97.4 |
fL |
| MCH |
27.3 |
25.9-32.7 |
pg |
| MCHC |
33.1 |
31.5-35.4 |
g/dL |
| RDW |
14.2 |
12.3-15.9 |
% |
| Platelet count |
228 |
153-369 |
10^3/uL |
| Immature Granulocytes |
3.9 H |
0.0-0.3 |
% |
| NUCLEATED RBCs |
0.2 |
|
% |
| Absolute neutrophil count |
6.25 |
1.50-7.50 |
10^3/uL |
| Absolute lymphocyte count |
1.25 |
1.10-3.40 |
10^3/uL |
| Absolute monocyte count |
1.02 |
0.30-1.10 |
10^3/uL |
| Absolute eosinophil count |
0.39 |
0.00-0.50 |
10^3/uL |
| Absolute basophil count |
0.02 |
0.00-0.30 |
10^3/uL |
| Band neutrophil |
0 |
0-5 |
% |
| Atypical lymphocytes |
3 |
0-6 |
% |
| Tear drop cells |
None |
|
|
| Platelet morphology |
Normal |
|
|
| DIFF TYPE |
Manual |
|
|
| Complete metabolic panel |
| Sodium |
136 |
(133-145) |
mmol/L |
| Potassium |
3.7 |
(3.5-5.0) |
mmol/L |
| Chloride |
98 |
(96-108) |
mmol/L |
| CO2 |
23 |
(22-29) |
mmol/L |
| Bun |
8 |
(6-20) |
mg/dL |
| Creatinine |
0.9 |
(0.7-1.2) |
mg/dL |
| Glucose |
103 |
(70-100) |
mg/dL |
| Calcium |
8.8 |
(8.6-10.0) |
mg/dL |
| Anion gap |
15 |
(7-17) |
|
| Calc osmolality |
281 |
|
mosm/kg |
| Bun/creat |
8 |
(5-28) |
|
| GFR african american |
>60 |
(>60) |
GFR UNIT |
| GFR non-african american |
>60 |
(>60) |
GFR UNIT |
| Bilirubin, total |
0.8 |
(<1.0) |
mg/dL |
| Total protein |
6.6 |
(6.4-8.3) |
g/dL |
| Albumin |
3.9 |
(3.5-5.2) |
g/dL |
| ALK PHOS |
52 |
(39-117) |
U/L |
| ALT |
32 |
(<42) |
U/L |
| AST |
37 |
(<39) |
U/L |
| Other chemistries |
| ANA screen |
Negative |
Negative |
|
| C reactive protein |
0.7 |
<0.5 |
mg/dL |
| Sed rate, erythrocytes ESR |
8 |
0-15 |
mm/hr |
Discussion
Vertebral Artery Dissection (VAD) occurs when the structural integrity of the arterial wall is compromised, leading to blood accumulation between the layers as an intramural hematoma. Although VAD is considered an uncommon cause of stroke in the general population, it is among the leading causes of ischemic stroke in individuals under 45 years of age [4]. Cervical spine manipulation has been associated with vertebral and carotid artery dissections, affecting both the cervical and cranial segments of these vessels [5]. While the estimated risk of vertebral artery dissection following spinal manipulation is approximately 1 in 20,000 manipulations, the exact incidence remains uncertain [6]. The overall incidence of cervical artery dissection is 4.69 per 100,000 person-years, with carotid artery dissection occurring at 2.43 per 100,000 person-years and vertebral artery dissection at 2.01 per 100,000 person-years, including cases linked to chiropractic adjustments [7].
VAD is typically triggered by varying degrees of head and neck trauma, which may or may not be associated with an underlying predisposition. Certain conditions, such as connective tissue disorders (e.g., fibromuscular dysplasia, Ehlers-Danlos syndrome, Marfan syndrome, and homocystinuria), as well as vascular abnormalities, increase susceptibility. Other risk factors include recent infections, hypertension, migraine, oral contraceptive use, and smoking [8]. Head and/or neck pain is the most common initial symptom, reported in 57% to 90% of cases. This pain is often severe, continuous, and of recent onset [9]. In a study involving 49 patients with cervical artery dissection, most individuals with head or neck pain presented within one to five days after symptom onset. Additional clinical features may include vertigo, unilateral facial paresthesia, cerebellar dysfunction, lateral medullary syndrome, and visual field defects [6]. However, identifying patients at risk for cerebral ischemia following cervical manipulation remains challenging, as no definitive clinical history or physical examination findings reliably predict such an outcome [10].
Magnetic Resonance Imaging (MRI) should include axial T1weighted, T2-weighted, Fluid-Attenuated Inversion Recovery (FLAIR), and diffusion-weighted sequences. Cervical and cranial T1-weighted MRI with fat saturation is particularly useful for detecting small intramural hemorrhages. For vascular imaging, contrast-enhanced Magnetic Resonance Angiography (MRA) and time-of-flight MRA can help confirm the diagnosis. Alternatively, CTA of the head and neck is a viable option. Conventional angiography (digital subtraction angiography) is reserved for cases where clinical suspicion remains high despite negative noninvasive imaging. Other diagnostic tools, such as carotid duplex and transcranial Doppler ultrasound, may be useful for monitoring treatment response. Angiographic findings indicative of VAD including the string sign, elongated tapered stenosis or flame-shaped occlusion, intimal flap, pseudoaneurysm, and intramural hematoma [11].
Although there is no definitive evidence favoring anticoagulation over antiplatelet therapy for stroke prevention following vertebral artery dissection [12], acute anticoagulation is commonly initiated using low-molecular-weight heparin (e.g., enoxaparin, dalteparin) or intravenous unfractionated heparin. Once the acute phase has passed, patients may be transitioned to warfarin in stable cases. For those who received anticoagulation in the acute setting, warfarin may be discontinued after six months in favor of long-term antiplatelet therapy, provided symptoms do not recur and follow-up imaging confirms thrombus resolution. If vascular imaging at three to six months reveals persistent luminal stenosis, irregularity, or dissecting aneurysm, continued anticoagulation may be considered. The use of direct oral anticoagulants in this setting remains an area of ongoing investigation [13]. Endovascular interventions, such as angioplasty, stent placement, embolization, or even surgical repair, may be considered in cases of recurrent ischemia despite optimal medical therapy [14].
One study examining chiropractic-related vascular injuries found that affected patients experienced milder neurological deficits at discharge and follow-up compared to non-chiropractic-associated cases. A greater proportion of patients who sustained chiropractic-related injuries had modified Rankin Scale (mRS) scores of 0-2 at discharge and at three-month follow-up with no reported cases of severe long-term deficits or mortality [15].
Conclusion
Vertebral artery dissection should be considered in patients presenting with new-onset headaches after cervical spine manipulation, as early recognition is crucial to preventing serious complications such as ischemic stroke. Prompt diagnosis using vascular imaging, including CTA or MRA, is essential for confirming the condition and guiding treatment. Although both anticoagulation and antiplatelet therapy are effective in preventing thromboembolic events, treatment should be individualized based on clinical presentation and imaging findings. Physicians should educate patients about the potential risks of chiropractic neck manipulation and recognize warning signs that warrant urgent evaluation. Increased awareness among healthcare providers is necessary to ensure timely intervention, reduce morbidity, and improve patient outcomes.
Learning objectives
• Recognize vertebral artery dissection as an important differential diagnosis in patients presenting with headaches, especially after recent neck manipulation or trauma.
• Understand the clinical presentation of vertebral artery dissection, including headache as a primary or sole symptom, with or without neurological deficits.
• Review current management strategies for vertebral artery dissection, including anticoagulation, antiplatelet therapy, and indications for endovascular or surgical intervention.
Author Declarations
Patient treated: Internal Medicine, Huntsville Hospital.
Financial support statement: No funding was required for this study.
Conflict of interest statement: We declare no conflict of interest.
Patient consent: Informed consent was obtained from the patient for publication of this case report and any accompanying images.
References
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018; 38: 1-211.
- Wang Z, Yang X, Zhao B, Li W. Primary headache disorders: From pathophysiology to neurostimulation therapies. Heliyon. 2023; 9: e14786.
- Zhu K, Born DW, Dilli E. Secondary Headache: Current Update. Headache. 2020; 60: 2654-2664.
- Britt TB, Agarwal S. Vertebral Artery Dissection. 2023 Mar 20. In: StatPearls. Treasure Island (FL): StatPearls Publishing. 2025.
- Albuquerque FC, Hu YC, Dashti SR, Abla AA, Clark JC, Alkire B, et al. Craniocervical arterial dissections as sequelae of chiropractic manipulation: patterns of injury and management. J Neurosurg. 2011; 115: 1197-205.
- Saeed AB, Shuaib A, Al-Sulaiti G, Emery D. Vertebral artery dissection: warning symptoms, clinical features and prognosis in 26 patients. Can J Neurol Sci. 2000; 27: 292-296.
- Griffin KJ, Harmsen WS, Mandrekar J, Brown RD Jr, Keser Z. Epidemiology of Spontaneous Cervical Artery Dissection: Population-Based Study. Stroke. 2024; 55: 670-677.
- Park KW, Park JS, Hwang SC, Im SB, Shin WH, Kim BT. Vertebral artery dissection: natural history, clinical features and therapeutic considerations. J Korean Neurosurg Soc. 2008; 44: 109-15.
- Manabe H, Yonezawa K, Kato T, Toyama K, Haraguchi K, Ito T. Incidence of intracranial arterial dissection in non-emergency outpatients complaining of headache: preliminary investigation with MRI/MRA examinations. Acta Neurochir Suppl. 2010; 107: 41-4.
- Haldeman S, Kohlbeck FJ, McGregor M. Unpredictability of cerebrovascular ischemia associated with cervical spine manipulation therapy: a review of sixty-four cases after cervical spine manipulation. Spine (Phila Pa 1976). 2002; 27: 49-55.
- Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. 2005; 352: 2618-2626.
- Arauz A, Ruiz A, Pacheco G, Rojas P, Rodriguez-Armida M, CantuC, et al. Aspirin versus anticoagulation in intraand extracranial vertebral artery dissection. Eur J Neurol. 2013; 20: 167-172.
- Serkin Z, Le S, Sila C. Treatment of Extracranial Arterial Dissection: the Roles of Antiplatelet Agents, Anticoagulants, and Stenting. Curr Treat Options Neurol. 2019; 21: 48.
- Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2021; 52: e364-e467.
- Cassidy JD, Boyle E, Cote P, Hogg-Johnson S, Bondy SJ, Haldeman S. Risk of Carotid Stroke after Chiropractic Care: A PopulationBased Case-Crossover Study. Journal of Stroke and Cerebrovascular Diseases. 2017; 26: 842-850.