Introduction
Biliary Atresia (BA) is a rare and stubborn disease, with a incidence rate ranging from 1/10000 to 1/16000 live births. Intracranial hemorrhage is one of the important causes of neurological dysfunction or death in newborns [3]. This article retrospectively analyzes the clinical data of a child with biliary atresia and intracranial hemorrhage admitted to Qingdao Women and Children’s Hospital, in order to accumulate experience for the understanding and treatment of such patients.
Case data
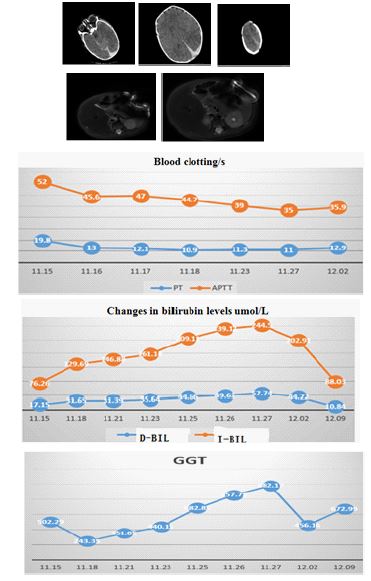
The patient, male, 29 days old, was admitted on November 14, 2022 due to “vomiting for 2 days, worsening accompanied by crying for 1 day, and convulsions once”. Admission physical examination: T36.2℃, P139 times/min, R16 times/min, Bp 90/62 mmHg, Weight 3.5 kg, in a calm state, with no yellowing of the skin, no rash or bleeding points throughout the body. The anterior fontanelle is 1.5×1.5 cm, swollen and has high tension. Bilateral pupils are equally large and round, with a diameter of about 3 mm, and slow to reflect light. Irregular breathing rhythm, inability to check limb muscle strength, increased muscle tone, warm extremities, CRT2 seconds. Coagulation routine: PT and APTT do not coagulate. Head CT scan shows:
1. Subdural hemorrhage in the left temporal and bilateral occipital regions.
2. Subarachnoid hemorrhage.
3. Median shift to the right.
Emergency subdural hematoma removal surgery+floating bone flap reduction surgery was performed. During and after the surgery, vitamin K1 was supplemented and plasma was infused to supplement coagulation factors. The child’s coagulation gradually improved and vital signs remained stable. After thinking about the poor coagulation function of the child after surgery, we found that the child’s liver function had a high level of direct bilirubin, and the color of the child’s stool was dark. Continuous monitoring of liver function changes revealed that direct bilirubin continued to rise, and biliary tract disease could not be ruled out. We requested a consultation with the neonatal surgery department to improve the abdominal MR prompt: 1. Insufficient gallbladder filling, small display, unclear display of the common bile duct. 2. A small amount of fluid accumulation around the liver. Pancreatic cholangiography (MRCP): The gallbladder and common bile duct are visible, and there is no significant dilation of the intrahepatic and extrahepatic ducts. On November 27, 2022, during the biliary exploration surgery, it was found that the cholangiography could not be visualized. Therefore, hepatic portal fibroplaque resection and hepatic portal jejunal Roux-en-Y anastomosis were performed. After the surgery, the child’s bilirubin gradually returned to normal. On December 12, 2022, the child has been followed up for one year and has since recovered well.
Discussion
Timely diagnosis of intracranial hemorrhage in infants and young children is crucial for the prognosis of their neurological recovery; Common clinical manifestations include poor breastfeeding, vomiting, drowsiness, convulsions, and swollen fontanelle. Therefore, for intracranial hemorrhage in infants and young children, close attention should be paid to the child’s consciousness and eating habits [4]; Incomplete myelination of the nervous system in infants and young children, intracranial hemorrhage, and increased intracranial pressure can stimulate and provoke the motor areas of the cerebral cortex, leading to epileptic seizures [5]. CT examination has high sensitivity and speed for intracranial hemorrhage. The CT scan of this child showed a large amount of subdural bleeding in the occipital and left parietal lobes, with swelling of brain tissue, disappeardisappearance of the ring pool, and unclear ventricles. Timely subdural hematoma removal surgery, floating reduction of bone flap, reduction of dura mater tension, and intracranial pressure implantation monitoring technology were performed. Intracranial pressure monitoring guided the child to safely and effectively reduce intracranial pressure, and floating reduction of bone flap avoided the economic burden of repairing after removing the bone flap [6].
The pathogenic factors of intracranial hemorrhage in infants and young children are often related to hypoxia, asphyxia, vascular malformation and rupture, coagulation dysfunction, and mechanical factors. The bleeding site is more common in the subarachnoid space; Premature infants (27-34 weeks) may experience significant subarachnoid hemorrhage due to hypoxia, and some severe cases may rupture into the ventricles, leading to ventricular dilation and even hydrocephalus; Full term infants are characterized by intraventricular choroidal plexus hemorrhage after hypoxia, which is more common within one week after birth. Subdural bleeding is often caused by mechanical factors during production; Intracranial hemorrhage in infants and young children is often caused by coagulation dysfunction, vitamin K deficiency, vascular malformation, and shaking syndrome. A rare case of intracranial hemorrhage caused by biliary atresia has been reported. The child in this case was born 29 days ago without a clear history of trauma. The patient had subdural hemorrhage and cerebral herniation, and timely surgical intervention gradually stabilized the condition. Preoperative examination assessed the possibility of bleeding caused by coagulation dysfunction.
Coagulation dysfunction is a common complication in children with biliary atresia, caused by bile acid accumulation that affects the absorption of fat-soluble vitamins, especially vitamin K, leading to vitamin K deficiency [9]. In addition, liver function damage caused by bile acid stasis also leads to impaired synthesis of vitamin K. Vitamin K deficiency leads to insufficient coagulation factors, which are necessary for the liver to synthesize coagulation factors II, VII, IX, and X [10]. When the child was admitted, APTT was unable to provide accurate results. Timely infusion of plasma improves coagulation function. Analysis shows that this child suffered from intracranial hemorrhage due to a lack of coagulation factors. Combined with persistent jaundice and significant increase in direct bilirubin, accounting for more than 50% of total bilirubin, GGT increased significantly, and stool showed white clay like changes. It is considered that liver function damage caused by biliary tract disease affects coagulation. A neonatal surgeon is requested to assist in diagnosis and treatment. Biliary tract exploration and angiography are performed to confirm biliary atresia, and timely hepatojejunostomy is performed to benefit the child. Although cases of intracranial hemorrhage caused by biliary atresia are rare, the treatment of intracranial hemorrhage in infants and young children should fully consider the cause of the bleeding, pay attention to etiological treatment, and improve the overall prognosis of the child.
References
- Hussein A, Wyatt J, Guthrie A, Stringer MD. Kasai portoenterostomy--new insights from hepatic morphology. J Pediatr Surg. 2005; 40: 322-326.
- Lykavieris P, Chardot C, Sokhn M, Gauthier F, Valayer J, Bernard O. Outcome in adulthood of biliary atresia: a study of 63 patients who survived for over 20 years with their native liver. Hepatology. 2005; 41: 366-371.
- Wu Yuxin. Research progress on the etiology of intracranial hemorrhage in full-term newborns [J]. Chongqing Medical Journal. 2022; 51: 2331-2335.
- Van Hasselt PM, de Vries W, de Vries E, et al. Hydrolysed formula is a risk factor for vitamin K deficiency in infants with unrecognized cholestasis. Pediatr Gastroenterol Nutr. 2010; 51: 773–6.
- Taylor A,Butt W,Rosenfeld J,et al, Arandomized trail of very early decompressive craniectomy in children with traumatic brain injury and sustained intracranial hypertension. Childs Nerv Syst. 2001; 17: 154-162.
- Deng Jingyang, Wu Liping, Cao Guobin, et al. Application of floating bone flap combined with dural decompression repair in cranial surgery. Chinese Journal of Neurosurgery. 2006; 5: 91-92.
- Matsuzaka T, Yoshinaga M, Tsuji Y, Yasunaga A, Mori K. Incidence and causes of intracranial hemorrhage in infancy: a prospective surveillance study after vitamin K prophylaxis. Brain Dev. 1989; 11: 384-388.
- Sato H, Node Y, Araki T, Ohhashi K, Harada N, Yamamoto Y: Intracranial hemorrhage due to vitamin K defi ciency associated with congenital biliary atresia: a case report. Neurosurg Emerg. 2000; 5: 77–80.
- Yanofsky RA, Jackson VG, Lilly JR, Stellin G, Klingensmith WC 3rd, Hathaway WE. The multiple coagulopathies of biliary atresia. Am J Hematol. 1984; 16: 171-80.
- He Shengfu, Wang Yuqin. Role of bile acids in cholestatic liver injury. Journal of Practical Hepatology. 2020; 23: 919-922.