Introduction
Meckel’s diverticulum, a remnant of the omphalomesenteric duct, is the most common congenital anomaly of the gastrointestinal tract, affecting about 2% of the population. Typically asymptomatic, it can, however, present with a range of complications, including diverticulitis, gastrointestinal bleeding, and bowel obstruction. The latter, while less common, can pose significant diagnostic and management challenges [1].
Small bowel obstruction secondary to Meckel’s diverticulum is relatively rare but clinically significant. The obstructive process may be due to various mechanisms such as volvulus, intussusception, enteroliths, or fibrous bands, making clinical diagnosis difficult. Symptoms often overlap with other acute abdominal conditions, which can delay appropriate intervention and increase the risk of complications [2].
While existing literature has documented cases of enteroliths within Meckel’s diverticulum dislodging and migrating distally to cause obstruction in the terminal ileum, to our knowledge, this case represents only the second reported instance of an enterolith remaining within the Meckel’s diverticulum itself, leading to mechanical obstruction.
This case report describes an extremely rare instance where an enterolith formed in a Meckel’s diverticulum caused a small bowel obstruction, detailing the patient’s clinical presentation, diagnostic process, and the subsequent surgical management. Through this case, we aim to underscore the importance of considering Meckel’s diverticulum in the differential diagnosis of small bowel obstruction and to provide insight into effective diagnostic and treatment approaches.
Case presentation
A 26-year-old female with a history of endometriosis presented with nausea and vomiting that have persisted for the past day. She described the onset of symptoms as sudden, occurring shortly after eating fast food, which she initially attributed to food poisoning. Her vomiting progressed to dry heaving, though her nausea began to improve following a dose of Reglan administered in the emergency department. Upon evaluation by the surgical team, she reported only residual chest soreness from the retching. She denied experiencing abdominal pain, fever, chills, or difficulty breathing. Her vital signs were within normal limits. Laboratory results were remarkable for WBC 13.2 with neutrophils of 89.3%.
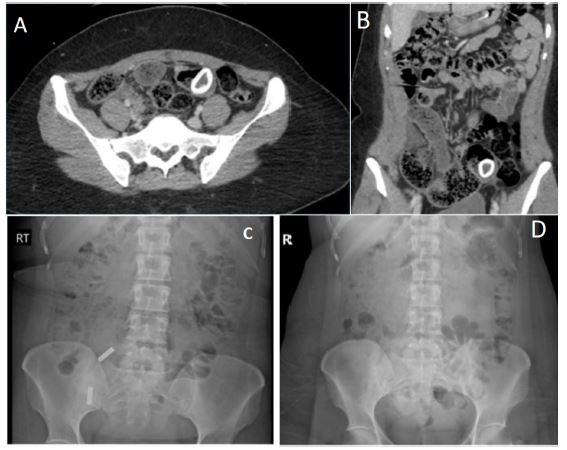
The patient stated that her last bowel movement was two days ago, though she had been passing flatus since then. A CT scan revealed dilation and fecalization of the small bowel, with the diameter reaching up to 4.4 cm, and identified a 2.8 cm radiodense foreign body within one of the distended loops of bowel. Despite this finding, the patient denied having ingested a foreign body. Her surgical history included a right salpingo oophorectomy due to Teratoma and torsion 1 year ago, and a left ovarian cystectomy.
On physical examination, the patient appeared well and in no acute distress. The abdomen was soft, non-distended, and mildly tender in the bilateral lower quadrants.
However, the patient noted that this tenderness was consistent with her baseline symptoms from previous ovarian surgeries. There was no guarding or rebound tenderness.
Initially, and given a relatively benign abdominal exam, the patient was managed conservatively with a regimen of NPO, intravenous fluids, pain control, and antiemetics. Given her lack of current nausea or vomiting, a nasogastric tube was deemed unnecessary and not placed.
After one day, the patient’s condition had not improved, and she had not had a bowel movement. To assess the status of the foreign body and determine if it was visible and in transit compared to the previous CT scan, an abdominal X-ray was obtained. An X-ray performed the previous evening did not reveal any foreign body (Figure 1).
The patient continued with an inability to tolerate the diet, prompting a decision to proceed with diagnostic laparoscopy, which revealed a Meckel’s diverticulum containing a large fecalith, necessitating conversion to open surgery with a supraumbilical mini laparotomy. Now extracorporeally, the diverticulum was mobilized, and the small bowel was transected proximally and distally using GIA staplers. A side-to-side anastomosis was performed. A nodularity on the proximal small bowel was excised and sent for pathology. The abdominal wound was closed with #1 Polydioxanone (PDS) sutures in a running fashion. The subcutaneous tissues were approximated using 3-0 Vicryl sutures, an adjacent lipoma was also excised. The skin was closed using a combination of 3-0 Vicryl and 4-0 Monocryl sutures in a subcuticular fashion. The patient tolerated the procedure well, without complications (Figure 2).
Immediately after surgery, she began with small sips of water. By postoperative day 1, she tolerated a clear liquid diet. By day 3, her bowel function returned and after successfully tolerating a regular diet, she was discharged home.
Discussion
Meckel’s diverticulum, present in about 2% of the population, is the most common congenital anomaly of the gastrointestinal tract [1]. Although often asymptomatic, it can lead to complications such as gastrointestinal bleeding, diverticulitis, and, rarely, small bowel obstruction [4].
The mechanisms of obstruction associated with Meckel’s diverticulum include volvulus, intussusception, enterolithiasis, and entrapment by fibrous bands. Diagnosing Meckel’s diverticulum preoperatively remains challenging, even with advanced imaging modalities like CT scans, and it is often discovered intraoperatively, as occurred in this patient [2].
Enterolithiasis occurs as a complication in 3-10% of cases of Meckel’s diverticulum. A large-scale study by Park et al. which examined 1,476 patients with this condition, revealed that 0.7% of those without symptoms and 6% of those with symptoms had enteroliths identified during laparotomy [3].
When considering the differential diagnosis for enterolithiasis, several possibilities should be included, such as a calcified abscess potentially linked to Crohn’s disease, an ingested foreign object, or bezoars. Other potential causes could be a calcified neoplasm or lymph node, gallstones, undescended testis, teratoma, or an abscess resulting from Crohn’s disease [5].
Enteroliths may lead to complications such as bowel obstruction, diverticulitis, bowel mucosal injury, perforation, afferent loop syndrome, intussusception, gangrene, hemorrhage, and iron deficiency anemia. Intestinal obstruction specifically due to enteroliths in Meckel’s diverticulum has rarely been reported [3].
To the best of our knowledge, this is only the second reported case of a large enterolith associated with Meckel’s diverticulum leading to small bowel obstruction at the site of the diverticulum itself. Typically, such enteroliths cause obstruction by dislodging from the diverticulum and migrating to the terminal ileum.
Surgical management is essential for symptomatic cases. The decision to perform a diverticulectomy or bowel resection depends on factors such as the extent of bowel involvement, inflammation, or ischemia. In this case, resection and primary anastomosis were necessary due to significant small bowel involvement, leading to a rapid and successful recovery [4].
Conclusion
This case highlights the importance of recognizing Meckel’s diverticulum as a potential cause of small bowel obstruction, especially in young adults with an unclear etiology. The presence of an enterolith in the diverticulum itself, rather than migrating distally, is a rare but clinically significant finding. Early diagnosis and timely surgical intervention are crucial in preventing complications. Given the diagnostic challenges associated with this condition, a high index of suspicion should be maintained when evaluating patients with unexplained small bowel obstruction [1,2].
Declarations
Conflicts of interest: The authors declare that there are no conflicts of interest regarding the publication of this case report.
Consent statement: Obtained written informed consent from the patient for the publication of any identifiable information, images, or case details.
References
- Hansen CC, Søreide K. Perforated Meckel’s diverticulum in adults: A scoping review of surgical management and patient outcomes. European Surgical Research. 2018; 59: 1–12.
- Kassahun WT, Fangmann J. Meckel’s diverticulum, a “simple” congenital anomaly that frequently becomes complicated. Journal of Gastrointestinal Surgery. 2021; 25: 2354–2362.
- Nastos C, Giannoulopoulos D, Georgopoulos I, Salakos C, Dellaportas D, Papaconstantinou I, et al. Large enterolith complicating a meckel diverticulum causing obstructive ileus in an adolescent male patient. Case Reports in Surgery. 2017; 2017: 1–3.
- Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: The Mayo Clinic experience with 1,476 patients (1950-2002). Annals of Surgery. 2005; 241: 529–533.
- Symeonidis N, Kofinas A, Psarras K, Pavlidis E, Pavlidis T. Meckel’s diverticulum enterolith: an extremely rare cause of intestinal obstruction. Journal of Clinical and Diagnostic Research. 2017.