Introduction
Filariasis is a common tropical disease caused by nematodes like Wucheria Bancrofti, Brugia Malai, and Brugia timori, transmitted by Culex mosquitoes. It presents acutely with fever, headache, and lymphadenitis, or chronically with lymphedema and hydrocoele. Diagnosis typically involves detecting microfilariae in blood smears. However rare, localised infections may be missed by conventional method.
Review of literature
Filarial granulomas are localized inflammatory reactions around filarial nematodes, caused by the host’s immune response to the worms or their secretions. These granulomas, involving eosinophils, macrophages, and sometimes neutrophils, develop in areas like the pleural cavity, lymphatics, and subcutaneous tissues. They are specific indicators of dead or degenerating Wuchereria Bancrofti worms, appearing as palpable lumps in clinical settings, such as in the scrotum of males with bancroftian filariasis. They can appear as palpable lumps, such as in the scrotum of males with bancroftian filariasis. All things considered, filarial granulomas are a major host reaction to filarial infections, entailing intricate interactions between the immune system and the parasite [1,2].
It is extremely uncommon for filariasis to manifest as subcutaneous nodules, and there are only very few documented examples in the literature.
Although Microfilaria Bancrofti is known to exist in a variety of locations, including the breast, thyroid, lymph nodes, liver, lungs, bodily fluids, and the scrotum, its presence in soft tissues is rarely documented, in contrast toother filarial species [3].
The conventional diagnosis of filariasis involves detecting microfilaria in peripheral blood smears, which can be diurnal or nocturnal [3,4]. Buffy coat is useful for detecting microfilaria in asymptomatic cases with eosinophilia. Species differentiation is based on morphological features like sheath presence, granules, and nuclear arrangement in the tail. A study by Kumar et al. (1998-2009) found among twenty-six filariasis cases diagnosed by FNAC, with nineteen related to Funiculo-epididymitis, four breast lumps, and three lymphadenopathies [5]. In twelve cases, smears showed adult worm fragments [5,6] including ten gravid female worm containing eggs and microfilariae and two male adult worms. The remaining fourteen cases had only microfilariae or eggs. Tissue responses included eosinophils (16 cases), acute inflammatory exudate (5 cases), macrophages (22 cases), epithelioid cell granulomas (5 cases), giant cells (4 cases), lymphocytes (10 cases), and plasma cells (3 cases). Polymorphonuclear leukocytes, eosinophils, and epithelioid cells adhered in four cases.
According to study by Pratima Khare, Pooja Kala, Aditi Jha, Nidhi Chauhan, Priyanka Chand out of swellings diagnosed as filariasis on FNAC majority were testiculo-scrotal followed by lymph node and thyroid [7]. On conclusion, filaria may affect the epididymis, spermatic cord, breast [3,5,6,8], and lymph node [3,5,7], thyroid [7] non-healing ulcers [9] and the accurate diagnosis can be easily and conveniently achieved by FNAC without any requirement of biopsy [5].
We hereby report a case series of filariasis whose initial clinical presentation was of asymptomatic subcutaneous nodules of few weeks to months duration over the upper limbs in which CBC, peripheral smear, and FNAC failed to identify filarial worm; later diagnosed on biopsy with histopathology sections showing gravid worm.
Materials and methods
Case series with supporting clinical examination and investigations such as complete Blood Count (CBC), ultrasonography (USG), FNAC, and histopathological examination.
Clinical scenario
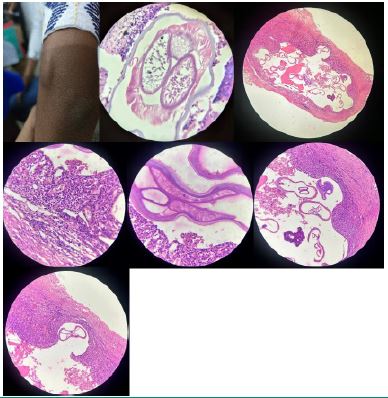
Case 1: A 59-year-old male with no comorbidities presented with generalized swelling in the left arm and forearm, which subsided on its own. He later noticed a pea-sized nodule over the BCG scar for three months. Examination revealed a one-by-one cm well-defined, firm, cystic lesion of left arm, spherical in shape, with smooth surface, skin above the swelling normal with no visible punctum, minimally fluctuant, mobile in all planes, firm in consistency with no signs of any inflammation in the subcutaneous plane. Basic blood workup such as CBC, viral markers, were normal. USG soft tissue showed cystic lesion with echogenic strands measuring twelve-by-six mm without significant vascularity. FNAC showed Fibro histiocytic lesion with cystic changes. Enucleation was performed, and histopathology confirmed a parasitic granuloma encasing a filarial worm. 12 am peripheral smear for microfilaria was negative. No evidence of eosinophilia. Patient was treated anti-filarial medications.
Case 2: A 9-year-old female with no known comorbidities presented with a one-month history of asymptomatic swelling in the left forearm. Examination revealed a 1x1 cm well-defined, firm, spherical swelling. Basic blood work was normal with 5% eosinophils. Sonography showed a cystic lesion. FNAC indicated chronic inflammation. The patient underwent excision under local anaesthesia, and histopathology confirmed a filarial granuloma encasing a gravid filarial worm. The peripheral smear was negative for parasites. The patient was treated with anti-filarial medications.
Case 3: A 37-year-old female with no known co-morbidities presented with a three-month history of asymptomatic swelling near the left elbow. Examination revealed a 1.5×2 cm well-defined, mobile, soft, ellipsoid swelling. Basic blood work was normal. Sonography showed well circumscribed ovoid homogenous lesion with scattered areas of thin septa within suggestive of lipoma. FNAC suggestive of polymorphous population of cells comprising neutrophils, lymphocytes, mononuclear cells, macrophages & histocytes and few plasma cells in necrotic background. Enucleation under local anaesthesia revealed a 1.5×1.5 cm cystic lesion. Histopathology reported as filarial granuloma encasing a gravid filarial worm. Peripheral smear was negative for microfilaria. The patient was treated with anti-filarial medications.
(Samples for peripheral smears of all patients were collected at 12 am and buffy coat was examined for microfilaria).
Discussion
This study emphasizes the clinical and histopathological features of subcutaneous filarial granulomas, highlighting the need to consider filariasis in the differential diagnosis of subcutaneous nodular masses, especially in endemic regions. The three cases presented demonstrate varied clinical presentations and the importance of histopathological examination for accurate diagnosis. The literature review supports the use of Fine Needle Aspiration Cytology (FNAC). Although FNAC did not show worm in our study other findings of FNAC were consistent with the literature. Histopathological examination was a crucial diagnostic tool, revealing fragments of adult worms and microfilariae. These findings underscore the critical role of histopathological examination in diagnosing filarial granulomas.
Strengths and weaknesses of the approach: The study’s strength is its detailed histopathological examination for diagnosing cutaneous filarial granulomas. However, its small sample size and retrospective nature limit capturing the full spectrum of clinical presentations.
Discussion of relevant medical literature: This study aligns with previous literature, emphasizing the diagnostic challenges and varied presentations of filarial infections. FNAC and histopathological examinations are crucial diagnostic tools, as supported by our findings.
Rationale of conclusion and primary takeaway: The study confirms that histopathological examination is the gold standard for diagnosing cutaneous filarial granulomas, with adult worms or microfilariae in tissue sections being definitive. Failure of conventional tools also suggests to the possibility that these nodules could be a local reaction to filarial remnants rather than active infection. It emphasizes considering filariasis in the differential diagnosis of subcutaneous nodular masses, especially in endemic regions. The primary takeaway is the need for high suspicion and thorough histopathological evaluation, as clinical, lab and imaging findings alone may not suffice. Failure of conventional tools also suggests to the possibility that these nodules could be a local reaction to filarial remnants rather than active infection. FNAC and histopathological examination are crucial, with treatment involving antiparasitic medications and surgical excision. Further research is needed on the topic.
Results and conclusion
In differential diagnosis of various subcutaneous nodular masses, the possibility of filarial granuloma must be kept, and a careful search should be done for adult worm or microfilaria in the serial tissue sections. The diagnosis of cutaneous filarial granulomas requires a high index of suspicion, especially in patients from endemic areas. Histopathological examination remains the gold standard for diagnosis. Treatment typically involves antiparasitic medications and surgical excision of the granuloma.
References
- Rajan B, Ramalingam T, Rajan TV. Critical Role for IgM in Host Protection in Experimental Filarial Infection. J Immunol. 2005; 175: 1827–33.
- Dash Y, Ramesh M, Kalyanasundaram R, Munirathinam G, Shultz LD, Rajan TV. Granuloma Formation around Filarial Larvae Triggered by Host Responses to an Excretory/Secretory Antigen. Infect Immun. 2010; 79: 838.
- Singh P, Chand N, Singal R, Madan M, Bala J. Filariasis presenting as multiple subcutaneous nodules: a rare case report. Acta Medica Indones. 2011; 43: 249–51.
- Ahuja M, Pruthi SK, Gupta R, Khare P. Unusual presentation of filariasis as an abscess: A case report. J Cytol Indian Acad Cytol. 2016; 33: 46.
- Kumar B, Karki S, Yadava SK. Role of fine needle aspiration cytology in diagnosis of filarial infestation. Diagn Cytopathol. 2011; 39: 8–12.
- Nanda A, Gupta N, Lamba S, Sethi D. Subcutaneous filariasis: An unusual presentation with an adult gravid worm on aspiration. Trop Parasitol. 2018; 8: 121–3.
- Khare P, Kala P, Jha A, Chauhan N, Chand P. Incidental Diagnosis of Filariasis in Superficial Location by FNAC: A Retrospective Study of 10 Years. J Clin Diagn Res JCDR. 2014; 8: FC05.
- Sodhani P, Murty DA, Pant CS. Microfilaria in a fine needle aspirate from a breast lump: a case report. Cytopathol Off J Br Soc Clin Cytol. 1993; 4: 59–62.
- Raghvendra G. Cytodiagnosis of filarial infection on a non healing ulcer: an unusual presentation and review of literature. 2012.