Introduction
Brain abscess is a rare and life-threatening central nervous
system infection, which is relatively uncommon in pediatric pa
t
ients. It is typically associated with conditions such as sinusitis,
otitis media, dermoid cysts, or head trauma, and is even rarer
in neonates, with the most common causes being meningitis
and septicemia. Dermoid Cysts (DCs) are relatively rare benign
tumors, accounting for 0.025% to 0.04% of all intracranial tu
mors. These cysts can become infected or rupture, leading to
complications such as headaches, seizures, chemical meningit is, neurological deficits, or hydrocephalus.
Case presentation
A 2-month-old male patient was admitted to the ICU in July
2024 due to feeding refusal and groaning for half a day. The
patient had a history of cesarean delivery at 28+4 weeks due
to threatened preterm labor and intrauterine infection. Fol
lowing admission, the patient’s condition rapidly deteriorated,
manifesting apnea, disturbed consciousness, weak spontane
ous breathing, and respiratory failure confirmed by blood gas
analysis. Treatment protocol included invasive mechanical ven
t
ilation, dobutamine for cardiac support, phenobarbital sodium
and midazolam for seizure control, and meropenem for infec
t
ion management. Physical examination revealed poor mental
response, grayish skin tone, respiratory distress, and a soft, flat
anterior fontanelle. Triple retractions were positive, with coarse
breath sounds and moist rales in both lungs, more prominent
in the right lung. The heart showed strong and regular beats
without significant murmurs. The abdomen was soft with the
liver palpable 3 cm below the costal margin and 2 cm below the
xiphoid, slightly firm, while the spleen was not palpable. Muscle
tone was normal with elicitable primitive reflexes. Laboratory
f
indings showed WBC 4.12×109/L, RBC 3.45×1012/L, hemoglobin
101.00 g/L, platelets 64.00×109/L, neutrophils 73.60%, and CRP
138.99 mg/L. Blood gas analysis indicated pH 7.299, PCO2
55.7
mmHg, PO2
45.6 mmHg, BE 0.0 mmol/L, K+ 5.7 mmol/L, Na+
140.0 mmol/L, and glucose 5.00 mmol/L. CSF analysis revealed
protein 196.03 mg/dl, chloride 114.7 mmol/L, glucose 2.63
mmol/L, WBC 1419.00×106/L, and nucleated cells 645.00×106/L.
Blood culture showed gram-negative bacilli, while sputum cul
ture identified Klebsiella pneumoniae and Staphylococcus au
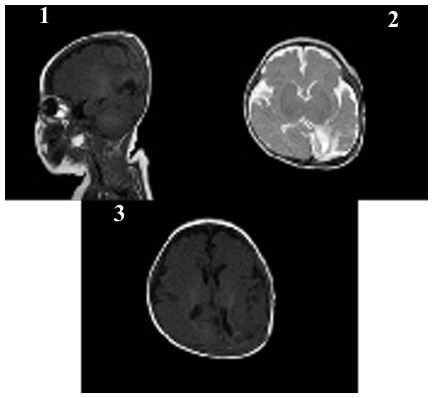
reus. Cardiac ultrasound demonstrated patent foramen ovale
and patent ductus arteriosus, while cranial ultrasound and MRI
showed no significant abnormalities. Diagnoses: 1. Neonatal
sepsis, 2. Neonatal purulent meningitis, 3. Neonatal pneumo
nia, 4. Septic shock, 5. Neonatal respiratory failure, 6. Cardiac
insufficiency, 7. Neonatal seizures, 8. Neonatal thrombocytope
nia, 9. Neonatal apnea.
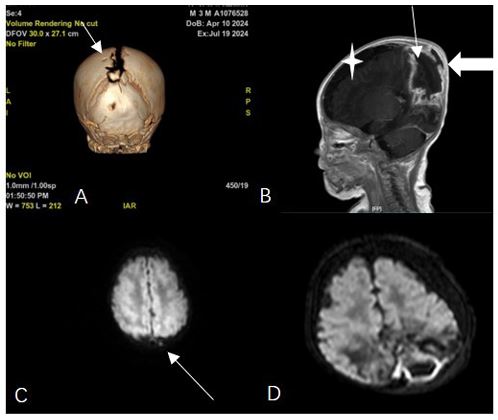
After 11 days of treatment, physical examination revealed
mild swelling and redness in the posterior fontanelle area at the
midline and slightly to the left of the occipitoparietal region, ap
proximately 3 cm in diameter, soft in texture with slight fluctua
t
ion. The brain enhanced MRI showed abnormal enhancement
signals in the right parietal lobe and the left parieto-occipital
area, suggesting an infectious lesion. Brain tissue was under
compression and midline shift were observed (Figure 1). After
the child was diagnosed with brain abscess, he was transferred
to the neurosurgery department for further treatment. The sur
gery of brain abscess drainage and external subdural effusion
drainage was performed under general anesthesia with tracheal
intubation. During the operation, a cyst infection was observed,
and it eroded the underlying dura mater, with tight adhesion
between the cyst wall, brain tissue, and dura mater surrounding the dura mater, thickening of the dura mater, and necrosis of the
surrounding brain tissue. The infected cyst wall was separated
from the surrounding dura mater, carefully dissected from the
lateral to the midline to the brain tissue interface, with protec
t
ion of the sagittal sinus at the midline, and deep erosion of the
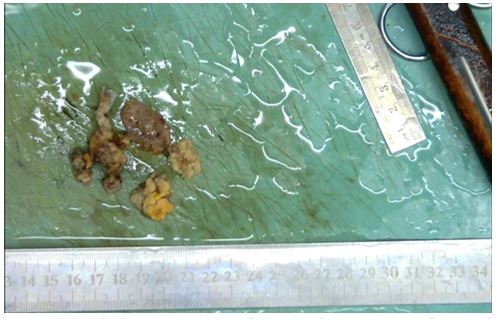
falx cerebri. The infected cyst had broken through to the oppo
site side. The right dura mater was incised, and the infected cyst
and necrotic brain tissue were thoroughly removed, connecting
both sides. The defected skull was about 1x3 cm in size (Figure
2). Infected DSTs and ruptured DCs with parieto-occipital brain
abscess were resected (Figure 3). Postoperative pathological
examination showed that purulent inflammation with abscess
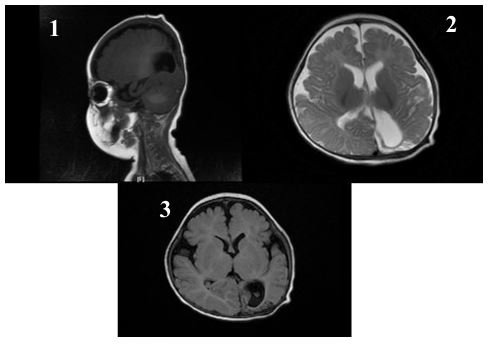
formation was formed. After surgery, the child was treated with
meropenem (0.2 g Q8H 21d) and linezolid (0.05 g Q8H 21d) to
resist infection. The child recovered smoothly after surgery, and
follow-up showed good growth, with no recurrence or neuro
logical sequelae (Figures 4 & 5).
Discussion
Dermoid Cysts are congenital developmental anomalies characterized by stratified squamous epithelial lining containing skin appendages (such as hair and sebaceous glands), and occasionally sweat glands, lymphoid tissue, and cartilage. Craniofacial dermoid cysts account for approximately 7% of all dermoid cysts, with an incidence rate between 0.03% and 0.14% [1]. Clinically, DCs often present insidiously, manifesting as fistulas, hemangiomas, or subcutaneous masses. Clinical symptoms typically include swelling, abnormal secretions, pain, and pruritus [2,3]. This case presents a rare vertex DCs, which was particularly challenging to diagnose as the initial physical examination revealed no subcutaneous mass or skin inflammation, making it exceptionally occult.
Once infected, skin microorganisms can enter the cyst through sinus tracts, leading to suppuration within the cyst, enlargement, and rupture. The cyst contents may then release into the ventricular system and subarachnoid space, spreading to the leptomeninges and causing purulent meningitis, which can result in complications such as sepsis, brain abscess, and hydrocephalus [2,4-6]. The main pathogenic organisms include Staphylococcus aureus, gram-negative bacilli, and anaerobic bacteria. In this case, gram-negative bacteria were identified in blood culture, likely associated with post-cyst infection sepsis. No bacterial growth was observed in the intraoperative pus culture, possibly due to prior sensitive antibiotic administration and culture condition limitations.
Neonatal brain abscesses can result from bacterial, fungal, or viral infections causing meningitis and sepsis [7]. Neonates with brain abscesses face a higher mortality risk, and survivors may experience permanent damage such as hemiplegia, epilepsy, and cognitive impairment [8]. Symptoms and signs in neonates and infants can be nonspecific and misleading. Clinical manifestations typically include fever, feeding refusal, irritability, lethargy, convulsions, and vomiting [9]. Due to the anatomical characteristics of open fontanelles and sutures in neonates, specific clinical manifestations like increased intracranial pressure may be absent, making the condition occult and prone to missed or delayed diagnosis. In this case, the patient showed no fever, sutural diastasis, or increased fontanelle tension, and the rapid disease progression was inconsistent with typical clinical presentations of brain abscess secondary to purulent meningitis. Therefore, for children with non-specific clinical manifestations, a high degree of clinical suspicion is crucial for early evaluation and timely medical and surgical management. Relevant imaging examinations should be conducted as early as possible.
The diagnosis of brain abscess can be made through cranial CT or MRI. CT scans are more effective for older children because the high-water content in the brains of newborns reduces the contrast between normal and affected tissues [10]. Enhanced MRI is the best method to prove the specific and non-specific expressions of intracerebral infectious inflammatory reactions, as it can more accurately determine the extended range of sinus tract extension and its relationship with abscesses, cysts, and venous structures. This imaging assessment is vital for early diagnosis and timely intervention. MRI typically shows ring-enhancing lesions on T1 scans after injecting contrast agents, and the DWI is shown on central high signal, with corresponding low ADC values. Dermoid cysts present as high signal on T1WI, and their signals on T22WI are variable, also showing high signal on DWI. Reviewing this patient’s cranial MRI at one month of age and comparing the same DWI plane at two months, the high signal observed at one month was likely a dermoid cyst that could be easily overlooked clinically. Therefore, we believe that for lesions especially near the midline, further neuroradiological examination is necessary to exclude potential DSTs and DCs.
Bodilsen et al. recommend that all patients undergo neurosurgical aspiration or brain abscess excision as soon as possible, if feasible (except for toxoplasmosis) [10]. We hold that surgery should be performed as early as possible once a diagnosis is confirmed, to completely remove the infected cyst and sinus tract. In principle, the abscess and cyst wall should be removed as thoroughly as possible to prevent the recurrence of the abscess. However, sometimes it is difficult to remove the cyst wall completely due to tight adhesion of the cyst capsule to important surrounding structures such as venous sinuses, and a small amount of cyst wall may remain. Subdural and subcutaneous drainage tubes should be placed to ensure adequate drainage at different levels, and postoperative standardized antibiotic therapy should be administered to resist infection.
Conclusion
This case demonstrates a rare presentation of vertex Dermoid Cysts (DCs) with intracranial extension and secondary infection, emphasizing the importance of early imaging for suspicious vertex DCs to identify intracranial extension. For intracranial lesions caused by this condition, aggressive surgical intervention with maximal lesion removal and layered drainage is recommended. This case report highlights the crucial role of accurate diagnosis and timely intervention in improving prognosis, while also reminding clinicians to carefully differentiate from complications of purulent meningitis when managing similar cases, and to implement appropriate treatment measures to prevent serious complications.
Declarations
Conflict of interest: There are no conflicts of interest to disclose concerning this study.
Funding: No funding was obtained for this study.
Ethics approval: Ethics approval and consent to participate.
Author contributions: For original article: Study conception and design: YY; data collection: XWC. analysis and interpretation of results: PZ, draft manuscript preparation: YY, YS. All authors reviewed the results and approved the final version of the article.
References
- Overland J, Hall C, Holmes A, Burge J. Risk of Intracranial Extension of Craniofacial Dermoid Cysts. Plast Reconstr Surg. 2020; 145: 779e-787e.
- Albastaki A, AlThawadi R, Alajaimi J, Ali KF, Almayman T. An Intracranial Extradural Dermoid Cyst Presenting with Two Dermal Sinuses and an Abscess in a Child. Case Rep Neurol Med. 2021; 2021: 9917673.
- Ségbédji FKK, Tokpo AJ, Nubukpo-Guménu AA, et al. Infected Intradural Dermoid Cyst with Complete Dermal Sinus of Posterior Fossa. World Neurosurg. 2018; 116: 219-224.
- Maaloul I, Hsairi M, Fourati H, Chabchoub I, Kamoun T, Mnif Z, et al. Occipital dermoid cyst associated with dermal sinus complicated with meningitis: A case report. Arch Pediatr. 2016; 23: 197-200.
- Raghunath A, Indira Devi B, Bhat DI, Somanna S. Dermoid cysts of the posterior fossa--morbid associations of a benign lesion. Br J Neurosurg. 2013; 27: 765-771.
- Gilard V, Beccaria K, Hartley JC, et al. Brain abscess in children, a two-centre audit: outcomes and controversies. Arch Dis Child. 2020; 105: 288-291.
- Pareek P, Gupta B, Chetan C, Banait N, Deshpande S, Joshi P, et al. Burkholderia cepacia Brain Abscess in a Term Neonate. Indian J Pediatr. 2020; 87: 478-479.
- Roos KL. Bacterial Infections of the Central Nervous System. Continuum (Minneap Minn). 2015; 21: 1679-1691.
- Bizubac M, Balaci-Miroiu F, Filip C, et al. Neonatal Brain Abscess with Serratia marcescens after Intrauterine Infection: A Case Report. Antibiotics (Basel). 2023; 12: 722.
- Bodilsen J, D’Alessandris QG, Humphreys H, et al. ESCMID Study Group for Infections of the Brain (ESGIB). European society of Clinical Microbiology and Infectious Diseases guidelines on diagnosis and treatment of brain abscess in children and adults. Clin Microbiol Infect. 2024; 30: 66-89.