Introduction
The occurrence of an umbilical hernia is a frequent reason for seeking surgical attention, often in non-emergent scenarios due to the presence of a lump at or adjacent to the umbilicus. However, instances also arise where emergency intervention becomes necessary, typically prompted by complications of obstruction or strangulation of herniated contents. Noteworthy risk factors associated with the development of umbilical hernias encompass female gender, obesity, and the presence of ascites [4].
A structural anomaly within the abdominal wall fascia situated at the umbilicus gives rise to an aperture through which intra-abdominal contents like preperitoneal adipose tissue, great omentum, or loops of the small or large intestine may protrude [6]. While omentum or bowel components are the prevailing contents of umbilical or paraumbilical hernias, infrequent occurrences involve the presence of epiploic appendages, or an inflamed vermiform appendix [1].
In the realm of hernias, those containing the appendix within the femoral (known as de Garengeot hernia) or inguinal (referred to as Amyand hernia) regions are more commonly documented [11]. Pertinently, while the inclusion of the appendix within a femoral or inguinal hernia has garnered greater attention, a limited documented instances exists within the medical literature elucidating the presence of an appendix-containing umbilical hernia. This case report endeavours to contribute additional insights and comprehensive information regarding this unusual and rare incidence.
Case presentation
A 63-year-old gentleman presented with a recurrent para-umbilical hernia, after an initial repair in 2013. The patient reported that the hernia had increased in size over the last three months, accompanied by worsening discomfort at the umbilicus, radiating to the epigastrium. Additionally, he observed slight changes on the surface skin surrounding the hernia. Upon further questioning, the patient reported constipation over the last two months, but denied experiencing nausea, vomiting, or chronic cough. The patient had a medical history of hypercholesterolemia treated with atorvastatin 20 mg and hypertension managed with amlodipine 10 mg. Also, past surgical history of enterogenous cyst repair in infancy and umbilical hernia repair in 2013. The patient denied any smoking or recreational drug use, reported consuming four bottles of wine per week. The patient’s job involves heavy lifting daily. No significant family history was known to the patient.
Physical examination revealed an obese middle-aged man in abdominal discomfort with blood pressure of 138/82, pulse of 78 beats/minute, tympanic temperature of 36.8oC, respiratory rate of 16 beats/minute, SpO2 of 95% and BMI 34.4 kg/m2. The abdominal examination showed a soft and non-tender abdomen, with mild sensitivity at palpation at the umbilicus and epigastric region. The umbilical hernia was irreducible, causing more discomfort than pain, especially during movements. The pre-operative images in (Figure 1) illustrate the clinical presentation of the umbilical hernia.
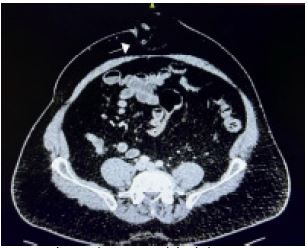
The CT report concluded: There is no free fluid in the abdomen and pelvis and no evidence of pneumoperitoneum. There is a substantial anterior abdominal wall midline hernia in the region of the umbilicus which contains non-compromised fat and the distal half of the appendix. The appendix does not appear particularly inflamed but the appendix within the hernial sac is dilated compared with the proximal appendix within the abdominal cavity which might imply a degree of obstruction at the level of the appendix entry into the hernial sac. (Figure 2) presents the CT imaging findings, demonstrating the presence of the appendix within the umbilical hernia.
Clinically was estimated that hernia was not complicated at the time of review and a delayed surgical repair of the hernia (with or without appendicectomy) was decided. Therefore, the patient was discharged on the day, with advice to avoid heavy lifting and was booked for an emergent elective procedure as a day case.
Three weeks later the patient was admitted for a day case operation. The laparoscopic approach was considered unsuitable by the anaesthetist due to ventilation-related concerns. Therefore, the patient underwent a Mayo hernia repair. The surgical procedure was initiated with infra-umbilical incision (“smile” skin incision), followed by dissection carried out in accordance with anatomical planes.
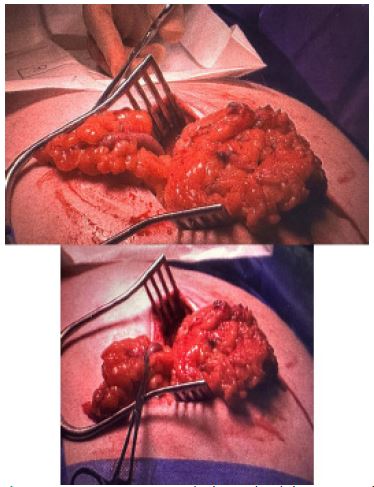
Intraoperatively, the identified findings consisted of a midline defect and a large hernial sac containing omental adipose tissue rapping around the terminal end of a normal appendix. Notably the end of an exceptionally long appendix, measuring approximately 30 cm, was situated within the hernial sac. This is demonstrated by intraoperative images on (Figure 3).
Through the hernial incision, it was attempted to mobilise the caecum and the appendiceal base in the operative field using an Alexis retractor, but it was impossible to accomplish this. As the tip of the appendix showed macroscopically normal appearance, the intention for appendicectomy was abandoned. The omentum and the appendix were separated under vision with haemostatic control and repositioned separately in the abdominal cavity. Subsequently, a Mayo repair was undertaken to address the defect.
The patient was discharged on the same day. The forthcoming objective for this patient entails the pursuit of an elective appendicectomy, contingent upon the outcome of pulmonary function assessments to evaluate potential undiagnosed manifestations of Chronic Obstructive Pulmonary Disease (COPD) and sleep apnoea.
Discussion
Recurrent umbilical and para-umbilical hernias may manifest with rare and atypical intra-hernial contents [5]. In this case, radiological assessment through CT imaging unveiled the pres
ence of the appendiceal tip within the confines of the hernial
sac, highlighting the diagnostic value of preoperative imaging in
identifying unexpected anatomical findings [7].
Intraoperatively, the appendiceal tip was found to be
wrapped by the omental tissue. Its skeletonization was con
ducted under direct vision, employing haemostatic measures
to ensure safe separation, consistent with established surgical
approaches for managing complex hernias [3].
In hindsight, a possible theory for this unique presentation
is that the patient had undergone an episode of early appen
dicitis, during which the omentum would have enveloped the
inflamed appendix as a protective mechanism to mitigate the
inflammation [2]. The considerable length of the appendix,
combined with its encasement by the omentum and its free
intra-abdominal mobility, likely facilitated the introduction of
the appendiceal tip into the hernial sac [9].
This clinical scenario demonstrates the pivotal role of radio
logical imaging in the context of recurrent hernias, given the
potential for unexpected contents. Without the pre-emptive
CT imaging that suggested the presence of the appendiceal tip
within the hernial sac, there existed a distinct likelihood of inad
vertent appendiceal transection during surgery. This could have
precipitated the formation of an intra-abdominal abscess and
engendered additional complexities in the overall management
of the patient’s condition [10].
Conclusion
The occurrence of an appendix in an umbilical hernia is a
rare pathology. The early diagnosis of such cases is essential to
reduce the risk of possible complications due to low incidence
and atypical presentation. This case also highlights the vital role
of preoperative CT imaging in recurrent abdominal hernias for
enhancing patient safety and optimising outcomes. By reveal
ing unexpected contents, such as the appendiceal tip in this
instance, CT imaging aided in precise surgical planning and re
duced the risk of complications during surgery, such as inadver
tent appendiceal injury. Incorporating CT imaging as a standard
preoperative practice in recurrent hernia cases not only safe
guards patients but also reflects modern healthcare’s commit
ment to providing the highest standard of care.
Declarations
Patient consent: Patient consent for the utilisation of CT im
aging and intra-operative images has been obtained. A corre
sponding consent form has been appended as supplementary
documentation. All additional patient-related information con
tained within this report has been anonymised for confidential
ity purposes.
References
- Agarwal N, Goyal S, Kumar A, Garg A, Kaur N, Gupta A. ‘Appen
dicitis in paraumbilical hernia mimicking strangulation: A case
report and review of the literature’. Hernia. 2013; 17: 531–532.
- Arroyo A, et al. ‘Management of uncommon hernia contents: A
surgical perspective’. Journal of Surgical Case Reports. 2019; 12:
234–238.
- Barut I, et al. ‘Intraoperative management of complex hernias
with atypical contents’. Hernia. 2020; 24: 987–993.
- Dabbas N, Adams K, Pearson K, Royle G. ‘Frequency of abdomi
nal wall hernias: Is classical teaching out of date?’. JRSM Short
Reports. 2011; 2: 1–6.
- Deeba S, et al. ‘Recurrent paraumbilical hernias with unexpect
ed intra-hernial pathology’. International Journal of Surgery.
2017; 45: 78–82.
- Doig CM. ‘Appendicitis in umbilical hernial sac’. BMJ. 1970; 2:
3–114.
- Ghosh S, et al. ‘CT imaging findings in rare cases of intra-hernial
appendiceal involvement’. Abdominal Imaging. 2011; 36: 157
162.
- Liang MK, Holihan JL, Itani K, Alawadi ZM, Gonzalez JR, Askenasy
EP, et al. ‘Ventral hernia management’. Annals of Surgery. 2017;
265: 80–89.
- Singh M, et al. ‘Unusual contents in hernial sacs: A case series’.
Journal of Clinical Surgery. 2015; 33: 123–127.
- Smith K, et al. ‘Postoperative complications following appendi
ceal injury during hernia repair’. American Journal of Surgery.
2018; 215: 341–346.
- Zormpa A, Alfa-Wali M, Chung A. ‘Appendicitis within the con
tents of an incarcerated paraumbilical hernia’. BMJ Case Re
ports. 2019: 12.