Introduction
Pneumoperitoneum due to Intestinal Cystic Pneumatosis (ICP) is a rare cause of pneumoperitoneum. It is characterized by the accumulation of gas in cystic cavities within the intestinal wall, primarily affecting the small intestine and colon [1]. Although most cases are asymptomatic, up to 30% may present with spontaneous pneumoperitoneum [2].
Diagnosis is based on radiological and endoscopic studies, which reveal the presence of air-filled cysts and pneumoperitoneum [3].
Medical treatment is indicated in most cases, including nasogastric decompression, oxygen therapy, antibiotics, and sclerotherapy. Surgery is required for complications such as obstruction, perforation, or hemorrhage [4].
Objective
Present a case report of this rare condition and its anatomical and radiological presentation through imaging findings.
Case report
A 76-year-old patient with a medical record of hypertension, coronary heart disease, epilepsy, atrial fibrillation, pacemaker use, retroperitoneal fibrosis due to IgG4-related disease, infrarenal abdominal aortic aneurysm treated through endovascular surgery, and hydronephrosis due to lithiasis treated with a pigtail catheter, presented to the emergency department with a one-week history of abdominal pain.
On admission, the patient was stable, mildly dehydrated and had abdominal pain without signs of peritoneal irritation. Laboratory findings included C-Reactive Protein (CRP) of 369.80 mg/L, creatinine of 1.82 mg/dL, and leukocyte count of 5,470/μL. Contrast-enhanced abdominal and pelvic Computed Tomography (CT) revealed extensive pneumoperitoneum in the upper right hemiabdomen, with no other significant findings.
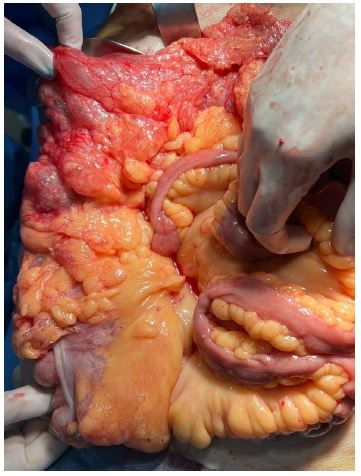
An exploratory laparotomy was performed, revealing inflammatory free fluid in the right paracolic gutter and pelvis, along with a small amount of free pneumoperitoneum. Extensive pneumatosis of the ascending colon and the right portion of the transverse colon was observed, extending into the retroperitoneum; however, the intestinal wall was intact, with no signs of ischemia. The rest of the colon appeared normal, with no other relevant findings. No resection was made and a 19F Blake drain was placed on the right paracolic gutter. The patient was treated with wide spectrum antibiotics and had a satisfactory clinical course, requiring no other intervention.
Results
The diagnosis of ICP is primarily radiological [1]. However, due to its rarity, its presentation with associated pneumoperitoneum can be mistaken for perforation of the gastrointestinal tract, leading to unnecessary surgical exploration [4]. The significance of our report lies in presenting a clinical case along with its characteristic anatomical findings to promote awareness of this condition and its appropriate management.
References
- Pascual Migueláñez I, Fernández Luengas D, Martínez Alegre J, Lima Pinto F, Torres Jiménez J. Características del neumoperitoneo por neumatosis quística intestinal. Gastroenterología y Hepatología. 2015; 38: 282–283.
- Boerner RM, Fried DB, Warshauer DM, Isaacs K. Pneumatosis intestinalis. Two case reports and a retrospective review of the literature from 1985 to 1995. Digestive diseases and sciences. 1996; 41: 2272–2285.
- Ling F, Guo D, Zhu L. Pneumatosis cystoides intestinalis: a case report and literature review. BMC gastroenterology. 2019; 19: 176.
- Peraza Casajús JM, Fernández F, Iglesias M, Montoro S, Borobia L. Neumoperitoneo espontáneo secundario a neumatosis quística intestinal [Spontaneous pneumoperitoneum secondary to intestinal cystic pneumatosis]. Cirugia espanola. 2009; 86: 113-114.